Dexamethasone versus betamethasone as an antenatal corticosteroid (ACS)
UN Commission / Born Too soon Care Antenatal Corticosteroids Working Group
Overview: Dexamethasone and betamethasone are the two antenatal corticosteroids (ACS) recommended for
accelerating fetal lung development in threatened preterm birth. The WHO, NIH, ACOG, RCOG, and WAPM list
both as effective drugs for preventing complications of prematurity, using either a dosage of 24 mg of
dexamethasone (4 doses of 6 mg 12 hours apart) or 24 mg of betamethasone (2 doses of 12 mg 24 hours apart).
Historical y, these drugs have often been used interchangeably, but betamethasone has sometimes been
preferred, as in the current WAPM guideline.
As of July 2013, the 18th list of WHO Model List of Essential Medicines, which includes ACS for the first time, lists
only dexamethasone for fetal indications.The Executive Summary of the WHO Expert Committee explains, “While
alternative steroids with similar efficacy were available, dexamethasone was considered the most appropriate
product based on availability and cost.”
A review of the comparative efficacy, safety, availability, and cost reveals why dexamethasone is often the best
choice for expanding the reach of life-saving ACS treatment.
1. Efficacy: Dexamethasone and betamethasone are equal y acceptable. Two Cochrane reviews found some
better outcomes for each drug, but both concluded further study would be needed to recommend one steroid as
superior to the other. A 2006 review of studies comparing ACS to control included 6 trials using dexamethasone
and 14 trials using betamethasone. Betamethasone was more effective in reducing RDS (44% vs 20%), while
reduction in mortality was similar (33% vs 28%).
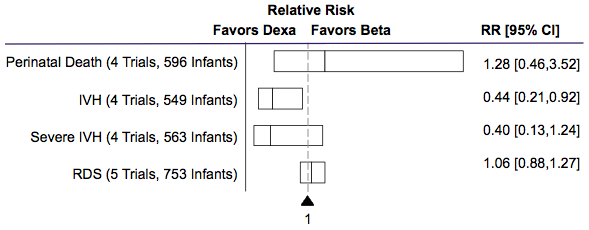
A 2008 Cochrane review of 9 studies directly comparing corticosteroids found substantial y greater reduction in
intraventricular hemorrhage (IVH) for dexamethasone, with no other statistical y significant difference in primary
outcomes, as shown below (not al studies reported al primary outcomes).
2. Safety: Dexamethasone and betamethasone are both acceptable. The 2006 review showed some elevated risks
for the mother from dexamethasone, particularly of puerperal sepsis, with a risk ratio of 1.74 [1.04 to 2.89]
compared to 1.00 [0.58 to 1.72] for betamethasone.However, neither review identified any other statistical y
significant differences in reported adverse effects. Despite potential y increased risk of maternal sepsis and fewer
trials for dexamethasone, Cochrane authors were able to conclude that antenatal dexamethasone is an overal safe
A large trial (A*STEROID) is underway to definitively compare the two drugs, with results expected in 2015. In the
meantime, as acknowledged in the WAPM as wel as RCOG, ACOG, and NIH guidelines, no definitive evidence
supports a clinical preference for either drug based on the balance of efficacy and safety outcomes.
3. Availability: The specific betamethasone used for fetal indications faces major supply shortages, dexamethasone is widely available. Not al injectable betamethasone is equivalent. The recommended
formulation for preterm birth is a less available mixture of long-acting betamethasone acetate (beta-ac) and fast-
acting betamethasone phosphate (beta-PO4). This mixture is used in the bulk of betamethasone trials, including 8
of 14 included in the 2006 Cochrane review (one used beta-PO4 only and 5 others used an unspecified
formulation). Though generic beta-PO4 injection is commonly available, data is limited to one trial vs control2 and
one comparative study of 69 infants which produced no statistical y significant results.6 Beta-PO 4is therefore not
The betamethasone (beta-ac+beta-PO4) used in most trials is best-known as Celestone®, with one comparably
priced generic identified from American Regent. Celestone has faced shortages in recent years, and manufacture
was suspended in 2004, both for reasons not specified by Merck, its manufacturer. American Regent reported
“sufficient inventory” as of July 23, 2013. Beta-ac+beta- PO4 is not sold at al in some countries, including India.
Dexamethasone sodium phosphate, in contrast, is available global y and from suppliers including UNFPA and
Mission Pharma among dozens of other vendors.Widespread availability is due in part to its use in many other
indications. Dexamethasone sodium phosphate is listed in four other sections of the current WHO EML3 and on
most national essential medicines lists.
4. Cost: A course of dexamethasone is far less expensive than a course of betamethasone
Depending on geography, a ful course of dexamethasone may cost around $1 USD, compared to over $35 for a
course of betamethasone (Celestone). Accounting for wastage due to non-optimal package size, a course of
dexamethasone stil costs less than 4% of the cost of a course of betamethasone. While dexamethasone requires
four injections compared to two for betamethasone, the cost of syringe, needle, and swab is relatively smal at
5. Summary: For treatment of women at risk of preterm delivery, dexamethasone is recommended over
betamethasone based on its efficacy, safety, wide availability, and low cost. While studies suggest some greater
risk of maternal sepsis, dexamethasone is overal a safe drug with better outcomes in reducing IVH and has been
found equal y acceptable for clinical use. Dexamethasone faces none of the supply problems of betamethasone
and is over 20 times cheaper per 24-mg course.
5 Dexamethasone vs betamethasone outcomes:
RDS: RR 0.80, 95% CI 0.68 to 0.93, 6 studies, 1457 infants vs RR 0.56, 95% CI 0.48 to 0.65, 14 studies, 2563 infants
NMR: RR 0.72, 95% CI 0.55 to 0.94, 6 studies, 1468 infants vs RR 0.67, 95% CI 0.54 to 0.82, 12 studies, 2488 infants
7 Dexamethasone vs betamethasone outcomes:
Puerperal sepsis: RR 1.74, 95% CI 1.04 to 2.89, 4 studies, 536 women vs RR 1.00, 95% CI 0.58 to 1.72, 4 studies, 467 women
Chorioamnionitis: RR 1.35, 95% CI 0.89 to 2.05, 4 studies, 575 women vs RR 0.71, 95% CI 0.50 to 1.01, 8 studies, 1910 women
STACI SAMPLE 123 Tivou Drive | Cedar Park, TX 78613 | (512) 555-9421 | [email protected] CANDIDATE: MEDICAL DEVICE SALES REPRESENTATIVE More than 10 years of experience exceeding sales targets for Core Competencies Include: a diverse range of companies with a proven record of hitting the ground running and producing immediate results. Experience leading new product launch
Special Purim Supplement Purim and Parody Like all the festivals of the Jewish calendar, Purim as we know it today is the product of a long history of development. Ostensibly a commemoration of national deliverance from danger, we should have expected solemn ceremonies of An exceptional passage in the "Bavli", the thanksgiving such as characterise Passover a
 Dexamethasone versus betamethasone as an antenatal corticosteroid (ACS)
Dexamethasone versus betamethasone as an antenatal corticosteroid (ACS)