Journal of the American College of Cardiology
2010 by the American College of Cardiology Foundation
The ARBITER 6-HALTS Trial(Arterial Biology for the Investigation of theTreatment Effects of Reducing Cholesterol 6 –HDL and LDL Treatment Strategies in Atherosclerosis)
Final Results and the Impact ofMedication Adherence, Dose, and Treatment Duration
Todd C. Villines, MD,* Eric J. Stanek, PHARMD,† Patrick J. Devine, MD,* Mark Turco, MD,‡Michael Miller, MD,§ Neil J. Weissman, MD,ʈ Len Griffen, MD,¶ Allen J. Taylor, MD*ʈ
Washington, DC; Franklin Lakes, New Jersey; and Takoma Park, Baltimore, and Rockville, Maryland
This report describes the final results of the ARBITER 6-HALTS (Arterial Biology for the Investigation of the Treat-
ment Effects of Reducing Cholesterol 6–HDL and LDL Treatment Strategies in Atherosclerosis) trial.
The ARBITER 6-HALTS trial was terminated early on the basis of a pre-specified interim analysis showing superi-
ority of niacin over ezetimibe on change in carotid intima-media thickness (CIMT). After termination, an addi-
tional 107 subjects completed a close-out assessment.
Patients with coronary heart disease (CHD) or CHD equivalent with low-density lipoprotein cholesterol Ͻ100mg/dl and high-density lipoprotein cholesterol Ͻ50 mg/dl for men or 55 mg/dl for women while receiving sta-ble statin treatment were randomly assigned to ezetimibe (10 mg/day) or extended-release niacin (target dose,
2,000 mg/day). The primary end point was change in mean CIMT, analyzed according to a last observation car-
ried forward method. The relationships of study medication adherence, dosage, and cumulative exposure (prod-
uct of adherence, dose, and time) with change in CIMT were explored.
Results in 315 patients included 208 with 14-month follow-up and 107 after mean treatment of 7 Ϯ 3 months. Niacin (n ϭ 154) resulted in significant reduction (regression) in mean CIMT (Ϫ0.0102 Ϯ 0.0026 mm; p Ͻ0.001) and maximal CIMT (Ϫ0.0124 Ϯ 0.0036 mm; p ϭ 0.001), whereas ezetimibe (n ϭ 161) did not reducemean CIMT (Ϫ0.0016 Ϯ 0.0024 mm; p ϭ 0.88) or maximal CIMT (Ϫ0.0005 Ϯ 0.0029 mm; p ϭ 0.88) com-pared with baseline. There was a significant difference between ezetimibe and niacin treatment groups on mean
changes in CIMT, favoring niacin, for both mean CIMT (p ϭ 0.016) and maximal CIMT (p ϭ 0.01). Increased cu-mulative drug exposure was related to regression of CIMT with niacin, and progression of CIMT with ezetimibe.
Niacin induces regression of CIMT and is superior to ezetimibe for patients taking statins.
2010;55:000–0) 2010 by the American College of Cardiology Foundation
Despite significant reductions in major cardiovascular
of ezetimibe or extended-release niacin (ERN) on carotid
events, lipid abnormalities and residual risk in patients
intima-media thickness (CIMT) in high-risk patients on
receiving statin monotherapy are prevalent We con-
stable, chronic statin monotherapy Results within the
ducted a comparative-efficacy trial examining the addition
initial 208 patients completing the 14-month trial demon-
From the *Cardiology Service, Walter Reed Army Medical Center, Washington, DC;
Stanek is an employee, with significant equity holdings, of Medco Health Solutions Inc.
†Medco Health Solutions, Franklin Lakes, New Jersey; ‡Washington Adventist Hospi-
Dr. Miller has received speaking honoraria from Merck. Dr. Turco received consulting
tal, Takoma Park, Maryland; §University of Maryland Medical Center, Baltimore,
fees and lecture honoraria from Abbott Cardiovascular. Dr. Taylor receives lecture
Maryland; ʈMedstar Research Institute, Washington Hospital Center, Washington,
honoraria from Abbott that are donated to charity. The opinions or assertions herein are
DC; and ¶Cardiac Associates, Rockville, Maryland. Abbott Pharmaceuticals funded
the private views of the authors and are not to be construed as reflecting the views of the
the study by an unrestricted, investigator-initiated research grant administered by the
Department of the Army or the Department of Defense.
Henry M. Jackson Foundation for the Advancement of Military Medicine, Rockville,
Manuscript received January 15, 2010; revised manuscript received February 26,
Maryland. Dr. Villines has received lecture honoraria from Novartis Pharmaceuticals. Dr.
Within-group comparisons of continuous variables were
performed using a paired t test or Wilcoxon signed-rank
test, as appropriate. A 2-sided p value Յ0.05 was considered
statistically significant. The SPSS for Windows version 16
software (SPSS, Chicago, Illinois) was used for all statistical
analyses. On the basis of a minimum sample size of 150 per
group, the trial had an 80% power to detect a difference of
CIMT change between agents of 0.02 Ϯ 0.06 mm/year
As previously described the study design pre-
HDL-C ؍ high-densitylipoprotein cholesterol
specified the performance of a blinded, interim analysis
according to the conservative method of O’Brien and
hsCRP ؍ highly-sensitiveC-reactive protein
Fleming with an alpha spending function, to be con-
ducted after 180 subjects (60% of the planned sample size)
had completed the trial. After the interim analysis (March
LDL-C ؍ low-densitylipoprotein cholesterol
2009), an independent data advisory committee (June 4,
2009) evaluated the primary end point data without knowl-
edge of treatment assignment, and based upon the trialfindings, unanimously recommended that the trial should beterminated.
After study termination on June 4, 2009, all actively
Patient population. The rationale, design, and primary
enrolled patients were contacted and returned for final
results of the ARBITER 6-HALTS study have been
collection of clinical variables, laboratory data, and blinded
described Briefly, inclusion criteria were as follows: 1)
CIMT assessment. Among the 363 patients initially en-
patients at least 30 years of age with known atherosclerotic
rolled in the trial, 208 patients had completed the entire 14
cardiovascular disease or coronary heart disease (CHD)
months of the study period at the time of their final visit
equivalent; 2) currently taking statin monotherapy at a
(111 ezetimibe, 97 ERN), and 44 had left the study. Final
consistent dose; 3) low-density lipoprotein cholesterol
ultrasound examinations could not be obtained in 4 addi-
(LDL-C) Ͻ100 mg/dl (2.6 mmol/l); and 4) high-density
tional subjects after termination of the study (total of 48
lipoprotein cholesterol (HDL-C) Ͻ50 mg/dl in men or
participants dropped out), leaving 315 patients for this
Ͻ55 mg/dl in women (1.3 or 1.4 mmol/l, respectively),
analysis. In 107 of the 315 patients analyzed, final achieved
documented on a lipid panel within 3 months of enrollment.
lipid values and CIMT measurements were performed after
Eligible patients were randomly assigned to open-label
study termination at a mean treatment duration of 7 Ϯ 3
therapy with either ezetimibe (10 mg/day) or ERN (target
months, and these values are included in the primary end
dose 2,000 mg/day). The ERN was initiated at 500 mg/day
point (a last observation carried forward analysis).
taken at bedtime, and increased by 500 mg every other weekto the maximum tolerated dose. There were no protocol-directed changes in statin medications or dosage throughout
the study. Adherence to study medication was determinedthrough tablet counts. The primary end point was the
The baseline characteristics of the 363 patients enrolled in
between-group difference in the change in mean CIMT
the trial were similar between the 2 treatment groups
A majority of the patients were male (80%), hypertensive
B-mode ultrasonography of the carotid arteries. Carotid
(87%), age 65 Ϯ 11 years, and had taken a statin (atorva-
ultrasound examinations were performed at baseline, 8
statin or simvastatin by 95%) at a mean dose of 42 mg for
months, and 14 months. We have previously described the
6 Ϯ 5 years. There was no difference with respect to age,
protocol for CIMT assessment utilized in this study
baseline lipid values, and CIMT between the 48 partici-
In summary, mean and maximal diastolic CIMT of the
pants who did not complete the trial and the remainder of
distal 1 cm of the far wall of the right and left common
the trial participants. In addition, there was no significant
carotid arteries was measured by a single, blinded, trained
difference among baseline covariates, including demograph-
observer utilizing an automated border-detection algorithm.
ics, blood pressure, lipid levels, baseline therapies, or base-
All images were obtained in duplicate, and no scans were
line CIMT between patients who completed the entire
excluded on the basis of image quality.
14-month trial (n ϭ 208) and patients who completed the
Statistical analysis. Between-group data for continuous
trial after study termination (n ϭ 107). Baseline and final
variables were evaluated using a t test for independent
lipid and biomarker values in the 315 patients who com-
variables or a Mann-Whitney U test, as appropriate. Cate-
pleted the trial are shown in Significant reductions
gorical variables were evaluated using the chi-square test.
in baseline LDL-C and triglycerides were seen with both
Randomly Assigned to Ezetimibe or Extended-Release Niacin
ACE ϭ angiotensin-converting enzyme; BMI ϭ body mass index; CHD ϭ coronary heart disease; CIMT ϭ carotid intima-media thickness.
ezetimibe and ERN. As compared with ERN, patients
Treatment with ezetimibe (n ϭ 161) had no effect on mean
treated with ezetimibe achieved significantly lower total
CIMT (Ϫ0.0016 Ϯ 0.0024 mm; p ϭ 0.88) or maximal
cholesterol, LDL-C, and HDL-C, and had higher triglyc-
CIMT (Ϫ0.0005 Ϯ 0.0029 mm; p ϭ 0.88) compared to
eride values. There was no difference in baseline or final
baseline. There was a significant difference between the
fasting glucose values between the study groups. There was
ezetimibe and niacin treatment groups on the change in
no significant difference between groups in clinically di-
CIMT, favoring niacin for both mean CIMT (p ϭ 0.016)
rected changes in the statin drug or dose during the study.
and maximal CIMT (p ϭ 0.01) among the 315 patients
Mean study drug adherence rates over the duration of the
completing the trial. Imputing baseline CIMT as the final
study exceeded 80% in each arm, and were significantly
CIMT (last observation of baseline CIMT carried forward)
higher with ezetimibe as compared with ERN (87.5 Ϯ
in the 48 patients who did not complete the trial resulted in
15.3% vs. 82.1 Ϯ 17.2%, respectively; p ϭ 0.005). Primary end point. The primary end point was assessed Impact of cumulative drug exposure. Based on differences
among all randomized subjects (n ϭ 315) who completed a
in study medication adherence, ERN dosage achieved and
final CIMT measurement after either 14 months (n ϭ 208)
treatment duration (due to early trial termination) between
or after Ͻ14 months of treatment (n ϭ 107) among subjects
trial participants, we performed an exploratory analysis to
who had not yet completed the study at the time of its
assess the impact of these variables on change in CIMT
termination Treatment with niacin (n ϭ 154)
among niacin and ezetimibe treatment groups. The product
resulted in significant reduction (regression) in mean CIMT
of study drug adherence, dosage, and treatment duration
(Ϫ0.0102 Ϯ 0.0026 mm; p Ͻ 0.001) and maximal CIMT
was calculated to estimate cumulative exposure to study
(Ϫ0.0124 Ϯ 0.0036 mm; p ϭ 0.001) compared to baseline.
drug as an integrated measure of drug effect The
Serum Biomarkers at Baseline and Study Completion
Serum Biomarkers at Baseline and Study Completion
Values are mean Ϯ SD. Median values listed with (interquartile range).
HDL-C ϭ high-density lipoprotein cholesterol; hsCRP ϭ highly-sensitive C-reactive protein; LDL-C ϭ low-density lipoprotein cholesterol.
relationships between increasing cumulative drug exposure
(lowest, quartile 1, to highest, quartile 4) and change inmean CIMT for all subjects using the method of last
We recently demonstrated that ERN leads to significant
observation carried forward are shown in and
regression of CIMT and was superior to ezetimibe when
Increased cumulative drug exposure resulted in regression of
added to chronic statin therapy among 208 high-risk
CIMT with niacin, and progression of CIMT with
patients who had completed 14 months of randomized,
ezetimibe. Specifically, comparing participants treated op-
open-label, parallel group treatment in the ARBITER
timally (best-case comparison), defined as those with the
6-HALTS trial This comparative-efficacy trial was
highest quartile of study drug adherence and those reaching
stopped before all enrolled patients completing the intended
the target 2,000 mg/day in the niacin group (quartile 4) for
14 months of drug treatment after a planned interim
the entire 14 months of the study, patients treated with
analysis clearly demonstrated the superiority of ERN over
ERN had significant reduction (regression) of mean CIMT
ezetimibe in the effect on CIMT. In the current analysis, we
from baseline (Ϫ0.0128 Ϯ 0.0078 mm), whereas patients
extend our original observations by examining the effect of
treated with ezetimibe experienced CIMT progression
the study treatments on CIMT within a last observation
carried forward and therapy optimization analysis.
Subjects and for All Subjects With the Last Observation Carried Forward
CIMT ϭ carotid intima-media thickness.
Change From Baseline CIMT Stratified by Quartiles of Increasing Cumulative Drug Exposure* to Ezetimibe and Niacin
Change From Baseline CIMT Stratified by Quartiles of Increasing Cumulative Drug Exposure* to Ezetimibe and Niacin
CIMT p value, ezetimibe vs. niacin within quartile
*Cumulative drug exposure ϭ (adherence ϫ dose ϫ treatment duration). Adherence, dose, and treatment duration expressed as mean Ϯ SD; CIMT expressed as mean Ϯ SE.
ANOVA ϭ analysis of variance; CIMT ϭ carotid intima-media thickness.
Consistent with the results seen for patients completing
effect between the 2 treatment strategies originally observed.
14 months of treatment, among the entire study group (n ϭ
This is a noteworthy possibility within the trial design of
315) including 208 subjects treated for the full study
ARBITER 6-HALTS with an 8-week titration period for
duration and 107 subjects treated for a mean of 7 months,
ERN to the target dose of 2,000 mg/day, as opposed to
therapy with ERN led to significant regression of baseline
ezetimibe, which was initiated at the maximal clinical dose.
CIMT among statin-treated patients with an LDL-C
Final results confirm the difference in the primary outcome
Ͻ100 mg/dl and an HDL-C Ͻ50 or 55 mg/dl. Treatment
and preserved magnitude of CIMT regression among pa-
with ezetimibe did not significantly change CIMT. Com-
tients taking ERN. In addition, the magnitude of effect of
paratively, there was a significant difference between the
ERN on mean CIMT, producing regression (Ϫ0.0142 Ϯ
effect of niacin and ezetimibe on changes in CIMT,
0.0041 mm), over 14 months of treatment in the relatively
favoring niacin. These results strengthen the findings from
high risk ARBITER 6-HALTS study population is note-
the interim analysis through the inclusion of patients treated
worthy in comparison with other contemporaneous lipid-
for shorter times (last observation carried forward analysis),
lowering trials using similar CIMT methodology. In the
which might have been expected to reduce the magnitude of
METEOR (Measuring Effects of Intima-Media Thickness:
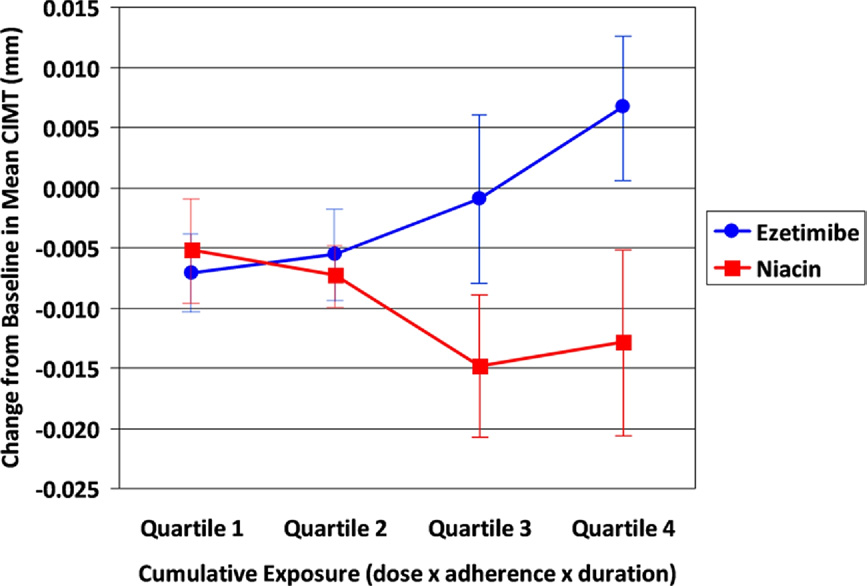
Relationship Between Quartiles of Cumulative Drug Exposure to Ezetimibe and Niacin and Change in CIMT
Cumulative drug exposure was calculated as the product of mean study drug adherence, dose, and time in the study. The relationship between quartiles of drug expo-
sure (lowest, quartile 1, to highest, quartile 4) and change in mean carotid intima-media thickness (CIMT) for all subjects using the method of last observation carried
forward is shown. The relationship between quartiles of cumulative drug exposure and change in CIMT is shown separately for ezetimibe (blue line) (analysis of variance
[ANOVA] p ϭ 0.05), and niacin (red line) (ANOVA p ϭ 0.23).
An Evaluation of Rosuvastatin) trial, treatment for 24
the end point of change in CIMT and the ability of niacin
months with high-potency statin monotherapy (rosuvastatin
to induce CIMT regression. Increased cumulative drug
40 mg; mean final LDL 78 mg/dl) in a low-risk population
exposure was related to regression of CIMT with niacin,
resulted in a change in mean common CIMT of 0.0004 mm
and progression of CIMT with ezetimibe.
(95% confidence interval: Ϫ0.0011 to 0.0019 mm), ascompared to placebo 0.0088 mm (95% confidence interval:
Reprint requests and correspondence: Dr. Todd C. Villines,
Cardiology Service, Walter Reed Army Medical Center, 6900
The observation that the CIMT response was related to
Georgia Avenue, NW, Building 2, Room 4A-34A, Washington,
niacin adherence, dose, and increased treatment duration,
calculated as cumulative drug exposure, is consistent with adrug effect as shown in prior studies demonstrating afavorable impact of niacin on clinical events and atheroscle-
rosis A prior study has shown regression of CIMTwhen ERN adherence rates are high, even when the dose
1. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of
was Ͻ2,000 mg/day Additional studies examining the
cholesterol-lowering treatment: prospective meta-analysis of data from90,056 participants in 14 randomised trials of statins. Lancet 2005;
optimal and minimal effective dose of ERN on atheroscle-
rosis, and ultimately clinical events, are warranted.
2. Devine PJ, Turco MA, Taylor AJ. Design and rationale of the
The relationship between cumulative drug exposure and
ARBITER 6 trial (Arterial Biology for the Investigation of the
the CIMT effect of ERN supports an expected, direct
Treatment Effects of Reducing Cholesterol)-6-HDL and LDL Treat-ment Strategies in Atherosclerosis (HALTS). Cardiovasc Drugs Ther
relationship between increasing intensity of drug exposure
(through a composite of dose, adherence, and time) and its
3. Taylor AJ, Villines TC, Stanek EJ, et al. Extended-release niacin or
effect on atherosclerosis. In contrast, findings with
ezetimibe and carotid intima-media thickness. N Engl J Med 2009;361:2113–22.
ezetimibe showing an unexpected inverse relationship be-
4. O’Brien PC, Fleming TR. A multiple testing procedure for clinical
tween intensity of drug exposure and CIMT draw further
trials. Biometrics 1979;35:549 –56.
attention to a growing body of evidence on the diverse
5. Holme I, Szarek M, Cater NB, et al. Adherence-adjusted efficacy with
effects of ezetimibe on cholesterol transport mechanisms,
intensive versus standard statin therapy in patients with acute myocar-dial infarction in the IDEAL study. Eur J Cardiovasc Prev Rehabil
such as interference with the pivotal HDL receptors SRB-1,
and ABCA1 Although the net health impact of
6. Crouse JR, III, Raichlen JS, Riley WA, et al. Effect of rosuvastatin on
ezetimibe’s described off-target receptor effects are yet to be
progression of carotid intima-media thickness in low-risk individualswith subclinical atherosclerosis: the METEOR trial. JAMA 2007;297:
fully understood, this evolving science clearly indicates that
the pharmacologic effects of ezetimibe extend beyond the
7. The Coronary Drug Project Research Group. Clofibrate and niacin in
simple inhibition of enteric cholesterol absorption, and
coronary heart disease. JAMA 1975;231:360 – 81.
8. Taylor AJ, Sullenberger LE, Lee HJ, Lee JK, Grace KA. Arterial
Biology for the Investigation of the Treatment Effects of Reducing
Study limitations. A limitation of this study is the use of
Cholesterol (ARBITER) 2: a double-blind, placebo-controlled study
CIMT as a surrogate for clinical end points. While the
of extended-release niacin on atherosclerosis progression in secondary
preponderance of studies demonstrate the validity of CIMT
prevention patients treated with statins. Circulation 2004;110:3512–7.
as a surrogate for cardiovascular events the
9. Taylor AJ, Lee HJ, Sullenberger LE. The effect of 24 months of
combination statin and extended-release niacin on carotid intima-
ultimate net health impact of therapeutics requires clinical
media thickness: ARBITER 3. Curr Med Res Opin 2006;22:2243–50.
end point trials. Additionally, our analysis evaluating cumu-
10. Kasza I, Hegyi Z, Szabo K, et al. Model system for the analysis of cell
lative drug exposure is post-hoc and exploratory in nature.
surface expression of human ABCA1. BMC Cell Biol 2009;10:93.
11. Labonte ED, Howles PN, Granholm NA, et al. Class B type I
Sample size is limited within ERN subjects who did not
scavenger receptor is responsible for the high affinity cholesterol
achieve the 2,000 mg/day target dose, and such subjects also
binding activity of intestinal brush border membrane vesicles. Biochim
were less adherent to the therapy. Prior studies in highly
adherent subjects treated for 1 to 2 years at the 1,000
12. Brown BG, Zhao XQ, Chait A, et al. Simvastatin and niacin,
antioxidant vitamins, or the combination for the prevention of coro-
mg/day dose showed regression of CIMT Dose-
nary disease. N Engl J Med 2001;345:1583–92.
ranging studies would be useful to further elucidate dose
13. Brown G, Albers JJ, Fisher LD, et al. Regression of coronary artery
disease as a result of intensive lipid-lowering therapy in men with highlevels of apolipoprotein B. N Engl J Med 1990;323:1289 –98.
14. Hodis HN, Mack WJ, LaBree L, et al. The role of carotid arterial
intima-media thickness in predicting clinical coronary events. AnnIntern Med 1998;128:262–9.
Final results from the ARBITER 6-HALTS trial confirmthe superiority of extended-release niacin over ezetimibe for
Key Words: atherosclerosis y risk factors y lipids.
The EFSA Journal (2007) 516 to 518, 1-12 Opinion of the Scientific Panel on food additives, flavourings, processing aids and materials in contact with food (AFC) on a request related to a 15th list of substances for food contact materials Question N° EFSA-Q-2005-253, EFSA-Q-2003-208, EFSA-Q-2006-049 Adopted on 3 July 2007 SUMMARY Within the general task of eva
Valentine’s Day Supper Menu, 2014 - £49.99 Tonight we celebrate the legend of Aphrodite, the Greek Goddess of Love and Beauty, the mother of Eros, and from whom the word Aphrodisiac was born. Every culture has it’s own unique twist on St. Valentine’s Day and true to our culture at the Olive Tree we have created our own bespoke menu, with 6 dishes each designed with their own ap
 Change From Baseline CIMT Stratified by Quartiles of Increasing Cumulative Drug Exposure* to Ezetimibe and Niacin
Change From Baseline CIMT Stratified by Quartiles of Increasing Cumulative Drug Exposure* to Ezetimibe and Niacin
CIMT p value, ezetimibe vs. niacin within quartile
*Cumulative drug exposure ϭ (adherence ϫ dose ϫ treatment duration). Adherence, dose, and treatment duration expressed as mean Ϯ SD; CIMT expressed as mean Ϯ SE.
Change From Baseline CIMT Stratified by Quartiles of Increasing Cumulative Drug Exposure* to Ezetimibe and Niacin
Change From Baseline CIMT Stratified by Quartiles of Increasing Cumulative Drug Exposure* to Ezetimibe and Niacin
CIMT p value, ezetimibe vs. niacin within quartile
*Cumulative drug exposure ϭ (adherence ϫ dose ϫ treatment duration). Adherence, dose, and treatment duration expressed as mean Ϯ SD; CIMT expressed as mean Ϯ SE.