010203 population screening in the age of genomic medicine
The new england journal of medicine
g e n o m i c m e d i c i n e
Alan E. Guttmacher, M.D., and Francis S. Collins, M.D., Ph.D., Editors
Muin J. Khoury, M.D., Ph.D., Linda L. McCabe, Ph.D.,
hysicians in the era of genomic medicine will have the oppor-
Prevention, Centers for Disease Control and
tunity to move from intense, crisis-driven intervention to predictive medicine.
Prevention, Atlanta (M.J.K.); and the De-partments of Human Genetics and Pedi-
Over the next decade or two, it seems likely that we will screen entire popula-
atrics, the David Geffen School of Medicine
tions or specific subgroups for genetic information in order to target interventions to
at UCLA, and the UCLA Center for Society,
individual patients that will improve their health and prevent disease. Until now, pop-
the Individual and Genetics, Los Angeles(L.L.M., E.R.B.M.). Address reprint requests
ulation screening involving genetics has focused on the identification of persons with
certain mendelian disorders before the appearance of symptoms and thus on the pre-
of Pediatrics, David Geffen School of Med-
vention of illness1 (e.g., screening of newborns for phenylketonuria), the testing of se-
icine at UCLA, 10833 Le Conte Ave., LosAngeles, CA 90095-1752, or at emccabe@
lected populations for carrier status, and the use of prenatal diagnosis to reduce the
frequency of disease in subsequent generations (e.g., screening to identify carriers ofTay–Sachs disease among Ashkenazi Jews). But in the future, genetic information willincreasingly be used in population screening to determine individual susceptibility tocommon disorders such as heart disease, diabetes, and cancer. Such screening willidentify groups at risk so that primary-prevention efforts (e.g., diet and exercise) orsecondary-prevention efforts (early detection or pharmacologic intervention) can beinitiated. Such information could lead to the modification of screening recommenda-tions, which are currently based on population averages (e.g., screening of people over50 years of age for the early detection of colorectal cancer).2
In this review, we describe current and evolving principles of population screening
in genetics. We also provide examples of issues related to screening in the era of ge-nomic medicine.
p r i n c i p l e s o f p o p u l a t i o n s c r e e n i n g
The principles of population screening developed in 1968 by Wilson and Jungner3form a basis for applying genetics in population screening. These principles empha-size the importance of a given condition to public health, the availability of an effectivescreening test, the availability of treatment to prevent disease during a latent period,and cost considerations. Wald outlined three elements of screening: the identificationof persons likely to be at high risk for a specific disorder so that further testing can bedone and preventive actions taken, outreach to populations that have not sought med-ical attention for the condition, and follow-up and intervention to benefit the screenedpersons.4 Several groups have used these principles to develop policies regarding ge-netic testing in populations.5 Screening of newborns, which has been carried out in theUnited States since the early 1960s, serves as a foundation for other types of geneticscreening.6,7
the diagnosis of sickle cell disease from four months
to two months.14 Rapid diagnostic confirmation is
Each state (and the District of Columbia) deter- imperative for the initiation of penicillin prophy-mines its own list of diseases and methods for the laxis to prevent illness and death in patients withscreening of newborns. Only phenylketonuria and sickle cell disease.15,16 The cost of this follow-uphypothyroidism are screened for by all these juris- test is $10 or less for each positive sample from thedictions.7 Table 1 lists the disorders that are includ- original screening.14ed in many state programs for newborn screening
Two-tiered testing is also used for congenital
and gives one an idea of the diversity of techniques hypothyroidism, since patients with primary hy-employed. The addition of a test or a method to a pothyroidism have elevated levels of thyrotropinstate’s screening program depends on the efforts and low levels of thyroxine.17,18 The two-tiered strat-of advisory boards for newborn screening, political egy provides better sensitivity and specificity thanlobbying of legislatures, and the efforts of labora- either test alone. However, the health care profes-tory personnel for newborn screening. There has sional needs to use clinical judgment in addition tooften been a lack of research to demonstrate the ef- the results of newborn screening. If a patient with afectiveness of screening and treatment for a disor- negative newborn-screening test has symptoms ofder, either before or after the disease is added to the congenital hypothyroidism, clinical acumen shouldnewborn-screening program. The technological override the test result and specific diagnostic test-spectrum ranges from the original Guthrie bacteri- ing should be performed.17 The results of screeningal inhibition assay, developed in the late 1950s,8 to tests are not infallible because of the possibility oftandem mass spectrometry9,10 and DNA analy- biologic, clerical, and laboratory errors.19-21sis.11-13 With the use of DNA testing of the blood
Audiometry is used to screen newborns for hear-
blot obtained from the screening of a newborn, the ing defects. The frequency of deafness in childhoodstate of Texas reduced the age at confirmation of is as high as 1 in 500.22 These programs are based
Table 1. Disorders Included in Newborn-Screening Programs. Disorder Screening Method Offering Test Treatment
Fluorescence assayAmino-acid analyzerTandem mass spectrometry
pneumoniae and Haemophilus
Vitamin B12 Diet restricting methionine and
The new england journal of medicine
in hospitals and are therefore decentralized.7 Mu-
A new form of technology, tandem mass spec-
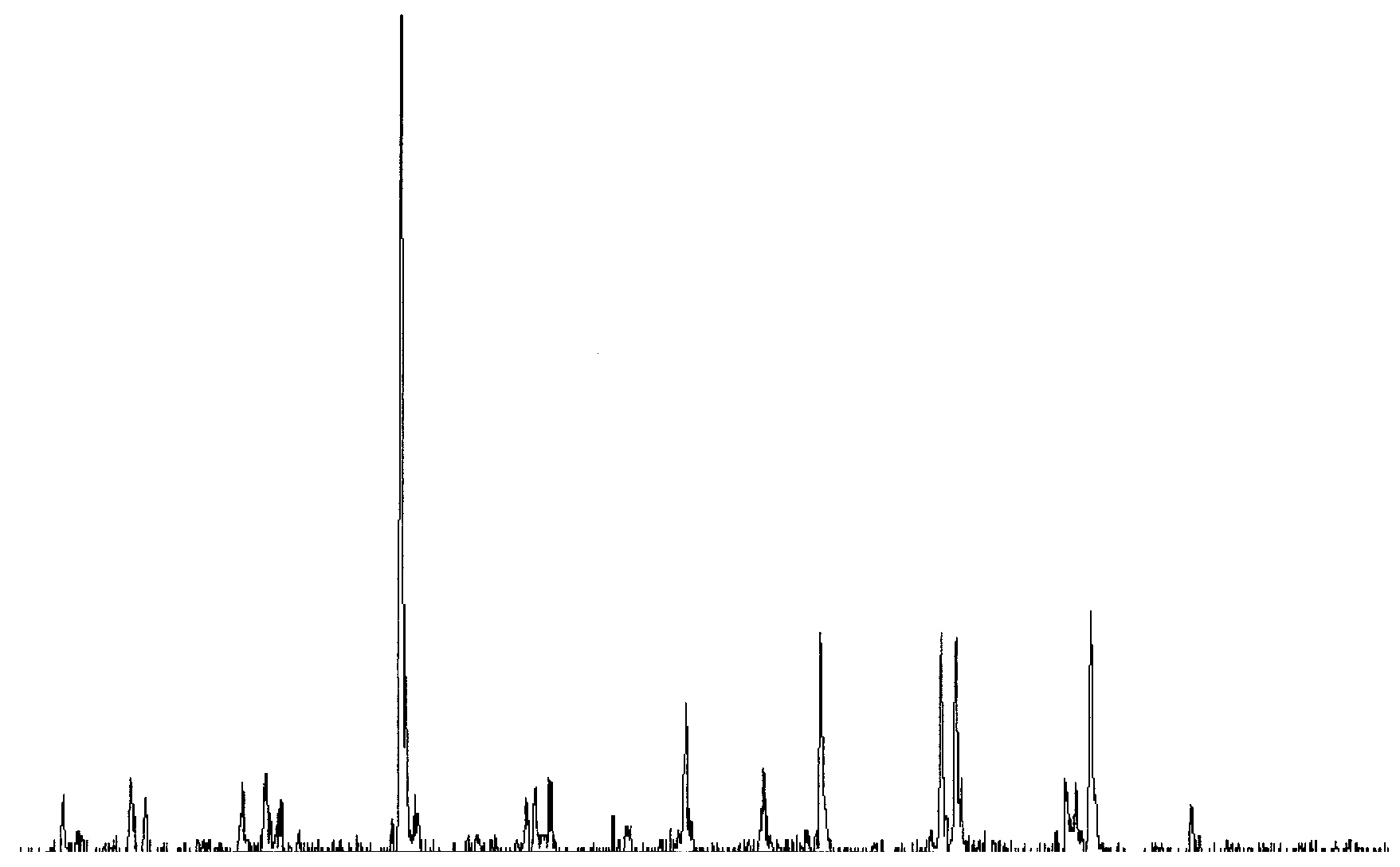
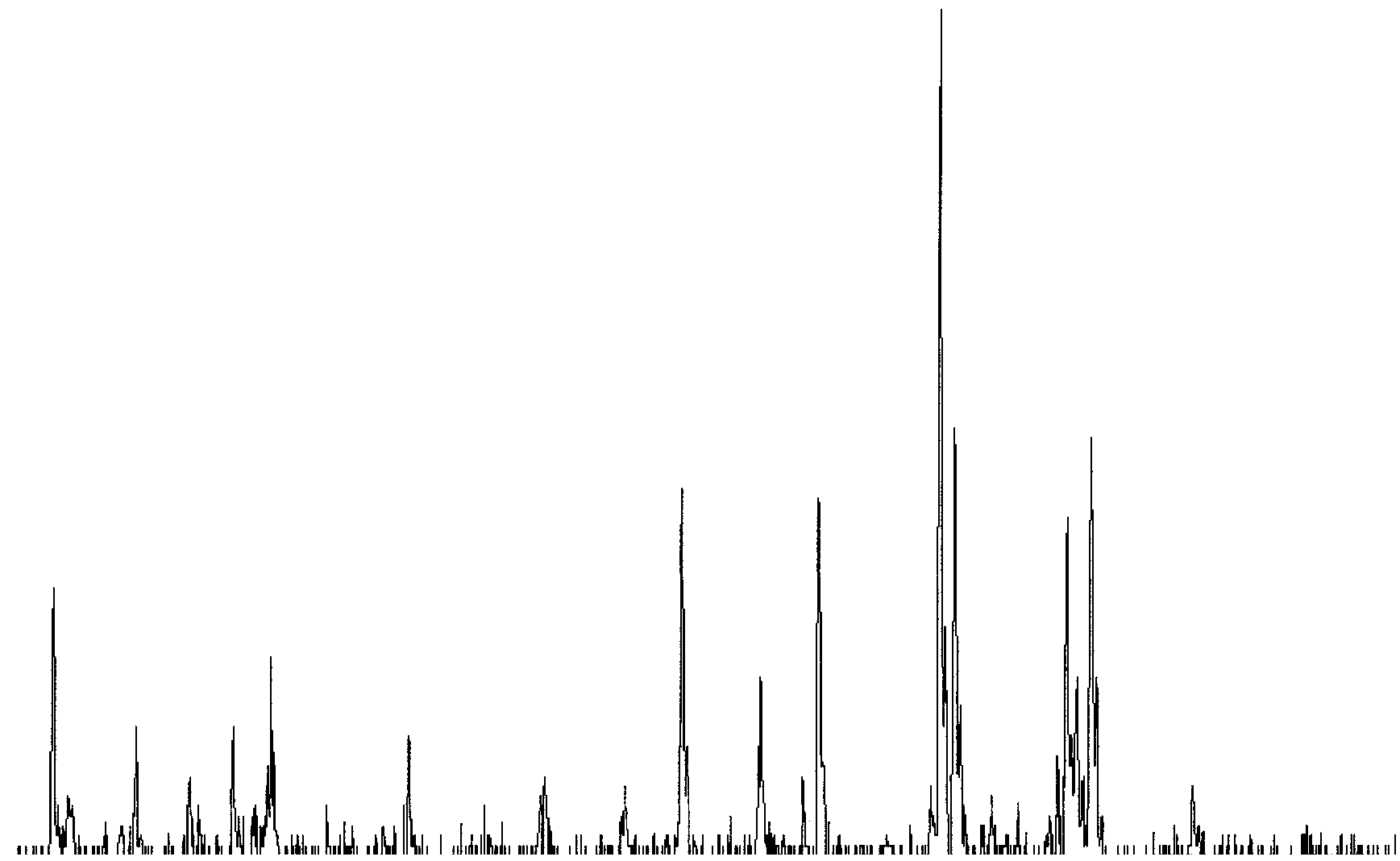
tations in the gene for connexin 26 account for 40 trometry, detects more than 20 disorders, not all ofpercent of all cases of childhood hearing loss, with which can be treated. A justification for introduc-a carrier rate of 3 percent in the population.23 A sin- ing tandem mass spectrometry is the identificationgle mutation is responsible for most of these cases of newborns with medium-chain acyl–coenzyme Ain a mixed U.S. population.23 A different mutation is (CoA) dehydrogenase deficiency (Fig. 1). Withoutpredominant among Ashkenazi Jews.24 Two-tiered early detection and intervention, this deficiencytesting in which audiometry is followed by DNA leads to episodic hypoglycemia, seizures, coma as-testing for mutations in the connexin 26 gene may sociated with intercurrent illnesses and fasting, andbe a useful and cost-effective approach to screen- a risk of death of approximately 20 percent after theing for hearing loss.25 Early detection provides the first episode in the first and second year of life.33,34possibility of aggressive intervention to improve a Management of medium-chain acyl–CoA dehydro-child’s language skills, provide cochlear implants, genase deficiency involves educating families aboutor do both.23
the dangers of hypoglycemia, which can be trig-
In 1999, the American Academy of Pediatrics gered by fasting, with resulting fat catabolism, dur-
and the Health Resources and Services Administra- ing intercurrent illnesses and by inadequate caloriction convened the Newborn Screening Task Force intake, and of the need for aggressive interventionto address the lack of consistency in the disorders with intravenous glucose if hypoglycemia does oc-included in screening programs and the testing cur. For many of the other disorders detected bymethods used in the various states.26 The group tandem mass spectrometry, treatment is not avail-concluded that there should be a national consen- able, but families will potentially be spared “diag-sus on the diseases tested for in state programs of nostic odysseys” with a severely ill child.35 The even-newborn screening. The American Academy of tual goal is collaborative research to determine thePediatrics, American College of Medical Genetics, appropriate treatment after early diagnosis.7,36 InHealth Resources and Services Administration, Cen- addition, this information may be useful for genet-ters for Disease Control and Prevention, March of ic counseling of these families. A cause for concernDimes, and other groups are working together to is that tandem mass spectrometry may detect met-create a national agenda for newborn screening.
abolic variations of unknown clinical significance,
A disorder that may be included in newborn creating unwarranted anxiety in parents and health
screening tests is cystic fibrosis. Cystic fibrosis has care professionals. been included in the newborn-screening programin Colorado since the demonstration that some af-
c a r r i e r s c r e e n i n g o f a d u l t
fected infants had malnutrition as a result of the
p o p u l a t i o n s f o r s i n g l e - g e n e
pancreatic dysfunction.27 This observation was con-
firmed by a randomized trial in Wisconsin involving infants with a positive newborn-screening test for tay–sachs disease cystic fibrosis.28 In the study, infants with a positive Carrier screening for Tay–Sachs disease has target- test were randomly assigned to a screened group ed Ashkenazi Jewish populations of childbearing (in which physicians were informed of the positive age.37 In a 30-year period, 51,000 carriers have been screening result) or a control group (in which phy- identified, resulting in the identification of 1400 sicians were informed of the positive screening re- two-carrier couples.37 Another approach has been sult when the child was four years of age if cystic fi- taken in Montreal, where high-school students learn brosis had not been diagnosed clinically or if the about Tay–Sachs disease and thalassemia as part of child’s parents had not asked about the results of a biology course. Those of Ashkenazi Jewish descent the screening test). In Wisconsin, infants are first tested with the use of an immunoreactive trypsino- gen assay29; if the result is positive, the test is fol- Figure 1 (facing page). Results of Screening by Tandem
lowed up with a DNA test of the original specimen
Mass Spectrometry for Medium-Chain Acyl–Coenzyme A (CoA) Dehydrogenase Deficiency in an Affected Patient
of dried blood obtained for newborn screening.30-32
(Panel A) and a Control Subject (Panel B).
The cost of each follow-up DNA test for infants with
IS denotes internal standard. (Figure provided courtesy
positive results on the immunoreactive trypsinogen
Intensity (counts/sec) Medium-Chain Acyl–CoA Dehydrogenase (mass-to-charge ratio) Intensity (counts/sec) Medium-Chain Acyl–CoA Dehydrogenase (mass-to-charge ratio) The new england journal of medicine
can request carrier testing for Tay–Sachs disease,
and those of Mediterranean ancestry can be tested
f o r g e n e t i c s u s c e p t i b i l i t y
for thalassemia.38 When women who have been
identified as carriers in high school later considerbecoming pregnant, they bring their partners in for Several groups have recently addressed the value oftesting. Although this program has been very suc- population screening for genetic susceptibility tocessful in Canada, the culture and the legal environ- conditions with onset in adulthood.46-48 Table 2 pre-ment in the United States, including a standard that sents a synthesis of the suggested modifications todoes not allow high-school students to consent to the 1968 criteria,3 based on current principles. medical care and the implications for insurability,
Hereditary hemochromatosis and the thrombo-
may prohibit the adoption of such a model.39
philia that results from carrying a single copy of afactor V Leiden gene are two adult-onset illnesses
c y s t i c f i b r o s i s
to which the suggested revised principles for popu-
Northern Europeans have a carrier frequency of lation screening would apply (Table 2), and these cystic fibrosis of 1 in 25 to 1 in 30; the rate is lower illnesses also reflect the complex scientific and so- in other ethnic and cultural groups.17 A 1997 Na- cial issues involved in screening for risk factors for tional Institutes of Health Consensus Development disease. As shown by Wald et al.,49 screening for Conference40 recommended that the following pop- risk factors for nondiscrete traits that are distrib- ulations be screened for mutations associated with uted continuously may not be beneficial even if the cystic fibrosis: the adult family members of patients factors are associated with a high risk of disease with cystic fibrosis, the partners of patients with (e.g., high cholesterol levels and heart disease). cystic fibrosis, couples planning a pregnancy, and This is because risk factors are determined by com- couples seeking prenatal care. Since more than 900 paring the probability of disease at each end of the different mutations associated with cystic fibrosis distribution of the risk factor (those with the high- have been reported in the literature,41 the establish- est level of risk and those with the lowest level of ment of screening programs has been difficult. risk). Those with a moderate level of risk are not However, the American College of Medical Genet- considered. The likelihood of a disorder, given a ics, the American College of Obstetricians and Gy- positive screening result, is expressed relative to the necologists, and the National Institutes of Health average risk of the entire population. The goal of agreed that mutations with a carrier frequency of at screening is to identify individual persons with a least 0.1 percent in the general population should high risk in comparison to everyone else. be screened for, resulting in a panel of 25 muta- tions recommended for carrier testing.42 These hereditary hemochromatosis guidelines suggest that carrier testing should be Many consider hereditary hemochromatosis to be offered to all non-Jewish white persons and Ashke- the key example of the need for population screen- nazi Jews and that other ethnic and cultural groups ing in the genomic era,50 but gaps in our knowledge should be informed of the limitations of the panel preclude the recommendation of population screen- to detect carriers in their group (in the case of black ing for this disorder. This policy issue was discussed persons) or of the low incidence of cystic fibrosis in by an expert-panel workshop held by the Centers their group (in the cases of Asian and Native Amer- for Disease Control and Prevention and the Nation- ican persons).
al Human Genome Research Institute.51 The panel
Mutations in the gene associated with cystic fi- concluded that population genetic testing for mu-
brosis have also been associated with obstructive tations in HFE, the gene for hereditary hemochro-azoospermia in men43 and with chronic rhinosi- matosis, could not be recommended because ofnusitis.44,45 The guidelines recommend including uncertainty about the natural history of the disease,in the screening panel a test for the R117H muta- age-related penetrance, optimal care for personstion, which is associated with congenital bilateral without symptoms who are found to carry muta-absence of the vas deferens.42 If the R117H muta- tions, and the psychosocial impact of genetic test-tion is found, further testing and genetic counsel- ing.52,53 On the other hand, mutation analysis maying are recommended.42
be useful in confirming the diagnosis of hereditaryhemochromatosis in persons with abnormal index-es of iron metabolism. A meta-analysis of studies54
showed that homozygosity for the C282Y mutationwas associated with the highest risk of hereditary
Table 2. Principles of Population Screening as Applied to Genetic Susceptibility to Disease.*
hemochromatosis. The risks associated with oth-er genotypes, including C282Y/H63D and H63D/
Public health assessment
H63D, were much lower. A recent large cohort study
The disease or condition should be an important public health burden to the target
population in terms of illness, disability, and death.
in the Kaiser Permanente Southern California health
The prevalence of the genetic trait in the target population and the burden of dis-
care network suggests that the disease penetrance
ease attributable to it should be known.
for HFE mutations may be quite low.
The natural history of the condition, from susceptibility to latent disease to overt
disease, should be adequately understood.
152 subjects who were homozygous for C282Y hadsymptoms of hereditary hemochromatosis. Evaluation of tests and interventions Data should be available on the positive and negative predictive values of the test
Several questions remain regarding the benefits
with respect to a disease or condition in the target population.
and risks of identifying and treating persons with-
The safety and effectiveness of the test and accompanying interventions should be
out symptoms who are at high risk for hereditary
hemochromatosis (i.e., through population screen-
Policy development and screening implementation
ing). This process should be clearly distinguished
Consensus regarding the appropriateness of screening and interventions for people
with positive and negative test results should be based on scientific evidence.
from early case finding, which could include testing
Screening should be acceptable to the target population.
of iron status, and analysis for mutations in HFE, in
Facilities should be available for adequate surveillance, prevention, treatment, edu-
persons who present with clinical symptoms con-
cation, counseling, and social support.
Screening should be a continual process, including pilot programs, evaluation of
sistent with a diagnosis of hereditary hemochro-
laboratory quality and health services, evaluation of the effect of screening, and
matosis. The natural history of hereditary hemo-
provisions for changes on the basis of new evidence.
chromatosis — particularly age-related penetrance
The cost effectiveness of screening should be established. Screening and interventions should be accessible to the target population.
— remains unknown. Despite the relatively high
There should be safeguards to ensure that informed consent is obtained and the
prevalence of the two most common mutations in
privacy of those tested is respected, that there is no coercion or manipulation,
and that those tested are protected against stigmatization and discrimination.
the nature and prevalence of mutations in specific * Principles are based on Wilson and Jungner,3 Goel,46 Khoury et al.,47 and
ethnic and cultural groups, as well as the morbid-
ity57 and mortality58 associated with this disease. Therefore, questions remain concerning the per- case–control study of risk factors for venous throm-sons most likely to benefit from early treatment bosis.66 Although the use of oral contraceptivesand thus about the optimal timing of screening and alone increases the risk of venous thrombosis by aeffective intervention, as well as ethical and psycho- factor of about 4 and the presence of factor V Leidensocial issues59 (Table 2).
alone increases the risk by a factor of about 7, theirjoint effect was an increase by a factor of more than
f a c t o r v l e i d e n
30. In spite of the high relative risk, the absolute
Factor V is an important component of the coagu- risk was relatively low (about 28 per 10,000 per-lation cascade leading to the conversion of pro- son-years) among women with factor V Leiden whothrombin into thrombin and the formation of used oral contraceptives, because the incidence ofclots.60 In factor V Leiden, the triplet coding for ar- this complication is relatively low in the population. ginine (CGA) at codon 506 is replaced by CAA,
The question of whether it is beneficial to screen
which codes for glutamine (R506Q), resulting in women for factor V Leiden before prescribing oralthrombophilia or an increased propensity for clot contraceptives remains controversial. Venousformation.61 The prevalence of factor V Leiden var- thrombosis is relatively rare, and the mortality as-ies.62,63 Among persons of northern European de- sociated with venous thrombosis is low amongscent, the prevalence is about 5 percent. The high- young women.67 More than half a million womenest prevalence of factor V Leiden is found in Sweden would need to be screened for factor V Leiden —and in some Middle Eastern countries; it is virtually resulting in tens of thousands of women beingabsent in African and Asian populations. Hetero- denied prescriptions for oral contraceptives — tozygosity for factor V Leiden results in an increase in prevent a single death. In addition to medical andthe incidence of venous thrombosis by a factor of financial considerations, there are issues related to4 to 9.64,65
the quality of life, the risk of illness and death from
An interaction between factor V Leiden and the unwanted pregnancy, and concern about possible
use of oral contraceptives was originally found in a discrimination by insurance companies. In 2001,
The new england journal of medicine
the American College of Medical Genetics stated unanticipated information that the opinions and practices regarding testing Misattribution of Paternity for factor V Leiden vary considerably, and no con- The American Society of Human Genetics has rec- sensus has emerged.68
ommended that family members not be informed
For the individual healthy woman contemplating of misattributed paternity unless determination of
the use of oral contraceptives, the risk–benefit equa- paternity was the purpose of the test.71 However, ittion does not currently favor screening. For wom- must be recognized that such a policy may lead toen without symptoms who have family histories of misinformation regarding genetic risk. multiple thrombosis, there are no evidence-basedguidelines, and decisions will have to be reached Unexpected Associations among Diseasesindividually, without reliance on population-based In the course of screening for one disease, informa-recommendations.
tion regarding another disease may be discovered.
These examples show why it is essential that Although the person may have requested screening
data continue to be analyzed to inform decision for the first disorder, the presence of the second dis-making for individual persons and populations.
order may be unanticipated and may lead to stigma-tization and discrimination on the part of insur-ance companies and employers. Informed consent
should include cautions regarding unexpected find-
The following are among the ethical, legal, and so- cial issues involved in population-based screening oversight and policy issues that confront health care providers, policymakers, In 1999, the Secretary’s Advisory Committee on Ge- and consumers.
netic Testing was established to advise the Depart-ment of Health and Human Services on the medical,
t e s t i n g c h i l d r e n f o r a d u l t - o n s e t
scientific, ethical, legal, and social issues raised by
d i s o r d e r s
the development and use of genetic tests (http://
Two committees of the American Academy of www4.od.nih.gov/oba/sacgt.htm).72 The commit-Pediatrics have recently addressed the issue of mo- tee conducted public outreach to identify issues re-lecular genetic testing of children and adolescents garding genetic testing. There was an overwhelm-for adult-onset disease.69,70 The Committee on Ge- ing concern on the part of the public regardingnetics69 recommended that persons under 18 years discrimination in employment and insurance. Theof age be tested only if testing offers immediate advisory committee recommended the support ofmedical benefits or if another family member ben- legislation preventing discrimination on the basisefits and there is no anticipated harm to the per- of genetic information and increased oversight ofson being tested. The committee regarded genetic genetic testing. The Food and Drug Administrationcounseling before and after testing as an essential was charged as the lead agency and was urged topart of the process.
take an innovative approach and consult experts
The Committee on Bioethics70 agreed with the outside the agency. The goal is to generate specific
Newborn Screening Task Force27 that the inclusion language for the labeling of genetic tests, much asof tests in the newborn-screening battery should be drugs are described in the Physicians’ Desk Reference.73based on evidence and that there should be in- Such labeling would provide persons considering,formed consent for newborn screening (which is and health professionals recommending, geneticcurrently not required in the majority of states). tests with information about the clinical validity andThe Committee on Bioethics did not support the value of the test — what information the test willuse of carrier screening in persons under 18 years provide, what choices will be available to peopleof age, except in the case of an adolescent who is after they know their test results, and the limits ofpregnant or is planning a pregnancy. It recom- the test. mended against predictive testing for adult-onset
In conclusion, although the use of genetic infor-
disorders in persons under 18 years.
mation for population screening has great poten-tial, much careful research must be done to ensurethat such screening tests, once introduced, will bebeneficial and cost effective. r e f e r e n c e s
Juengst ET. “Prevention” and the goals
fibrosis using immunoreactive trypsin. 15. Gaston MH, Verter JI, Woods G, et al.
Pediatr Pulmonol Suppl 1991;7:76-83.
Prophylaxis with oral penicillin in children
30. Seltzer WK, Accurso F, Fall MZ, et al.
for colorectal cancer. N Engl J Med 2002;
with sickle cell anemia: a randomized trial.
Screening for cystic fibrosis: feasibility of
molecular genetic analysis of dried blood
16. Consensus Development Panel. New-
practice of screening for disease. Public
born screening for sickle cell disease and
health papers no. 34. Geneva: World Health
31. Gregg RG, Wilfond BS, Farrell PM, Lax-
Wald NJ. The definition of screening.
tion of DNA analysis in a population-screen-
ing program for neonatal diagnosis of cystic
17. American Academy of Pediatrics Com-
fibrosis (CF): comparison of screening pro-
public health genetics policy development.
mittee on Genetics. Newborn screening fact
tocols. Am J Hum Genet 1993;52:616-26.
In: Khoury MJ, Burke W, Thomson EJ, eds. 32. Kant JA, Mifflin TE, McGlennen R, Rice
Genetics and public health in the 21st cen-
18. Burrow GN, Dussault JH, eds. Neonatal
E, Naylor E, Cooper DL. Molecular diagno-
tury: using genetic information to improve
thyroid screening. New York: Raven Press,
sis of cystic fibrosis. Clin Lab Med 1995;15:
Oxford University Press, 2000:61-82. 19. McCabe ERB, McCabe L, Mosher GA, 33. Roe CR, Ding J. Mitochondrial fatty acid
Allen RJ, Berman JL. Newborn screening for
oxidation disorders. In: Scriver CR, Beaudet
phenylketonuria: predictive validity as a
programs, principles, and research. Wash-
function of age. Pediatrics 1983;72:390-8.
& molecular bases of inherited disease. 8th
ington, D.C.: National Academy of Sciences,
20. Holtzman C, Slazyk WE, Cordero JF,
McCabe LL, Therrell BL Jr, McCabe ERB. 34. Matsubara Y, Narisawa K, Tada K, et al.
Newborn screening: rationale for a compre-
genital hypothyroidism. Pediatrics 1986;78:
hensive, fully integrated public health sys-
21. Dequeker E, Cassiman J-J. Quality eval-
uation of data interpretation and report-
nine method for detecting phenylketonuria
ing. Am J Hum Genet 2001;69:Suppl:438. 35. Wilcken B, Travert G. Neonatal screen-
in large populations of newborn infants.
ing for cystic fibrosis: present and future. 22. Mehl AL, Thomson V. The Colorado 36. Naylor EW, Chace DH. Automated tan-
1992–1999: on the threshold of effective
ciency: quantitative analysis of octanoylcar-
screening for disorders in fatty acid, organic
nitine and other acylcarnitines in newborn
ing screening. Pediatrics 2002;109:134.
blood spots by tandem mass spectrometry. 23. Cohn ES, Kelley PM. Clinical phenotype 37. Kaback MM. Population-based genetic 10. Andresen BS, Dobrowolski SF, O’Reilly
and mutations in connexin 26 (DFNB1/GJB2),
screening for reproductive counseling: the
Tay-Sachs disease model. Eur J Pediatr 2000;
ing loss. Am J Med Genet 1999;89:130-6.
MS/MS-based prospective screening of new-
24. Morrell RJ, Kim HJ, Hood LJ, et al. 38. Mitchell JJ, Capua A, Clow C, Scriver CR.
borns differ from those observed in patients
Mutations in the connexin 26 gene (GJB2)
with clinical symptoms: identification and
characterization of a new, prevalent muta-
recessive deafness. N Engl J Med 1998;339:
b-thalassemia disease carriers in high
tion that results in mild MCAD deficiency.
schools. Am J Hum Genet 1996;59:793-8. 25. McCabe ERB, McCabe LL. State-of-the- 39. McCabe L. Efficacy of a targeted genetic 11. McCabe ERB, Huang S-Z, Seltzer WK,
art for DNA technology in newborn screen-
ing. Acta Paediatr Suppl 1999;88:58-60.
blood spots on filter paper blotters: poten-
26. Newborn Screening Task Force. Serving 40. Genetic testing for cystic fibrosis:
tial applications to newborn screening.
the family from birth to the medical home:
12. Jinks DC, Minter M, Tarver DA, Vander-
future — a call for a national agenda on state
genetic testing for cystic fibrosis. Arch
ford M, Hejtmancik JF, McCabe ERB. Molec-
ular genetic diagnosis of sickle cell disease
41. Grody WW, Desnick RJ. Cystic fibrosis 27. Reardon MC, Hammond KB, Accurso
population carrier screening: here at last —
FJ, et al. Nutritional deficits exist before
are we ready? Genet Med 2001;3:87-90.
2 months of age in some infants with cystic
42. Grody WW, Cutting GR, Klinger KW, 13. Descartes M, Huang Y, Zhang Y-H, et al.
fibrosis identified by screening test. J Pediatr
Richards CS, Watson MS, Desnick RJ. Labo-
ratory standards and guidelines for popula-
dried blood specimens in a neonatal hemo-
28. Farrell PM, Kosorok MR, Rock MJ, et al.
tion-based cystic fibrosis carrier screening.
Early diagnosis of cystic fibrosis through
neonatal screening prevents severe malnu-
43. Mak V, Zielenski J, Tsui L-C, et al. Pro- 14. Zhang Y-H, McCabe LL, Wilborn M,
trition and improves long-term growth. Pedi-
portion of cystic fibrosis gene mutations not
29. Hassemer DJ, Laessig RH, Hoffman GL,
improved follow-up in a neonatal hemoglo-
Farrell PM. Laboratory quality control issues
44. Raman V, Clary R, Siegrist KL, Zehn- 54. Burke W, Imperatore G, McDonnell SM,
bauer B, Chatila TA. Increased prevalence of
Baron RC, Khoury MJ. Contribution of dif-
mutations in the cystic fibrosis transmem-
ferent HFE genotypes to iron overload dis-
brane conductance regulator in children with
ease: a pooled analysis. Genet Med 2000;2:
64. Rosendaal FR, Koster T, Vandenbroucke
chronic rhinosinusitis. Pediatrics 2002;109:
JP, Reitsma PH. High risk of thrombosis in
55. Beutler E, Felitti VJ, Koziol JA, Ho NJ, 45. Wang XJ, Moylan B, Leopold DA, et al.
Gelbart T. Penetrance of 845G→A (C282Y)
(activated protein C resistance). Blood 1995;
Mutation in the gene responsible for cystic
HFE hereditary haemochromatosis muta-
fibrosis and predisposition to chronic rhi-
tion in the USA. Lancet 2002;359:211-8. 65. Emmerich J, Rosendaal FR, Cattaneo M,
nosinusitis in the general population. JAMA
56. Steinberg KK, Cogswell ME, Chang JC,
et al. Combined effect of factor V Leiden and
et al. Prevalence of C282Y and H63D muta-
46. Goel V. Appraising organised screening
tions in the hemochromatosis (HFE) gene in
programmes for testing for genetic suscep-
the United States. JAMA 2001;285:2216-22.
tibility to cancer. BMJ 2001;322:1174-8. 57. Brown AS, Gwinn M, Cogswell ME, 47. Khoury MJ, Burke W, Thomson EJ.
Genetics and public health: a framework for
morbidity in the United States: an analysis
the integration of human genetics into pub-
of the National Hospital Discharge Survey,
66. Vandenbroucke JP, Koster T, Briet E,
lic health practices. In: Khoury MJ, Burke W,
Reitsma PH, Bertina RM, Rosendaal FR. 58. Yang Q, McDonnell SM, Khoury MJ,
Increased risk of venous thrombosis in oral-
health in the 21st century: using genetic
contraceptive users who are carriers of fac-
information to improve health and prevent
associated mortality in the United States
disease. New York: Oxford University Press,
from 1979 to 1992: an analysis of Multiple-
Cause Mortality Data. Ann Intern Med 1998;
67. Vandenbroucke JP, van der Meer FJM, 48. Burke W, Coughlin SS, Lee NC, Weed 59. Imperatore G, Valdez R, Burke W. Case
Leiden: should we screen oral contraceptive
screening principles to genetic screening
for adult-onset conditions. Genet Test 2001;
68. Grody WW, Griffin JH, Taylor AK, Korf 49. Wald NJ, Hackshaw AK, Frost CD.
When can a risk factor be used as a worth-
while screening test? BMJ 1999;319:1562-5.
York: Oxford University Press (in press).
Leiden mutation testing. Genet Med 2001;3:
50. Collins FS. Keynote speech at the Sec- 60. Greenberg DL, Davie EW. Introduction
to hemostasis and the vitamin K-dependent
69. Committee on Genetics. Molecular
coagulation factors. In: Scriver CR, Beaudet
genetic testing in pediatric practice: a sub-
Office of Genetics & Disease Prevention,
ject review. Pediatrics 2000;106:1494-7.
2000. (Accessed December 6, 2002, at http:
& molecular bases of inherited disease. 8th
70. Nelson RM, Botkjin JR, Kodish ED, et al.
Ethical issues with genetic testing in pediat-
51. Cogswell ME, Burke W, McDonnell SM, 61. Esmon CT. Anticoagulation protein 71. The American Society of Human Genet-
C/thrombomodulin pathway. In: Scriver CR,
sis: a public health perspective. Am J Prev
Beaudet AL, Sly WS, Valle D, eds. The meta-
genetic research. Am J Hum Genet 1996;59:
bolic & molecular bases of inherited dis-
52. Burke W, Thomson E, Khoury MJ, et al.
ease. 8th ed. Vol. 3. New York: McGraw-Hill,
72. McCabe ERB. Clinical genetics: com-
passion, access, science, and advocacy. Genet
62. Rees DC, Cox M, Clegg JB. World distri-
based screening. JAMA 1998;280:172-8.
bution of factor V Leiden. Lancet 1995;346:
73. Physicians’ desk reference. 56th ed. 53. EASL International Consensus Confer-
Montvale, N.J.: Medical Economics, 2002. 63. Ridker PM, Miletich JP, Hennekens CH, Copyright 2003 Massachusetts Medical Society.
Buring JE. Ethnic distribution of factor V
Adipositas-Abstract-Service Kommentar: Dr. Andreas van Egmond-Fröhlich, SMZ Ost - Donauspital, Abteilung für Kinderheilkunde und Jugendmedizin, Langobardenstraße 122, 1220 Wien Smith, S. R., N. J. Weissman, et al. "Multicenter, placebo-controlled trial of lorcaserin for weight management." , N Engl J Med 363 (3): 245-56. Der ZNS-selektive Serotonin (5HT2C) Rezeptor Agonist
Introduction : présentation de NanoSMS (Jérémie Léonard, IPCMS) Surfaces fonctionalisées et nanostructurées pour applications biomédicales : Nadia Jessel, UMR 595, Faculté de Chirurgie Dentaire: « Nanostructured and Multilayered Active Materials for Clinical Applications” Lydie Ploux, ICSI, Mulhouse : « Adhésion de cellules osseuses humaines et de bactéries sur des surfac
 Intensity (counts/sec)
Intensity (counts/sec)