Additive Beneficial Effects of Losartan Combined With Simvastatin in the Treatment of Hypercholesterolemic, Hypertensive Patients
Kwang Kon Koh, MD; Michael J. Quon, MD, PhD; Seung Hwan Han, MD; Wook-Jin Chung, MD;
Jeong Yeal Ahn, MD; Yiel-Hea Seo, MD; Moon Ho Kang, MD; Tae Hoon Ahn, MD;
Background—Biological mechanisms underlying statin and angiotensin II type 1 receptor blocker therapies differ.
Therefore, we compared vascular and metabolic responses to these therapies either alone or in combination inhypercholesterolemic, hypertensive patients. Methods and Results—This was a randomized, double-blind, placebo-controlled crossover trial with 3 treatment arms
(each 2 months) and 2 washout periods (each 2 months). Forty-seven hypertensive, hypercholesterolemic patients weregiven simvastatin 20 mg and placebo, simvastatin 20 mg and losartan 100 mg, or losartan 100 mg and placebo dailyduring each 2-month treatment period. Losartan alone or combined therapy significantly reduced blood pressurecompared with simvastatin alone. Compared with losartan alone, simvastatin alone or combined therapy significantlychanged lipoproteins. All 3 treatment arms significantly improved flow-mediated dilator response to hyperemia anddecreased plasma malondialdehyde and monocyte chemoattractant protein-1 levels relative to baseline measurements. However, these parameters were changed to a greater extent with combined therapy compared with simvastatin orlosartan alone (both PϽ0.001 and Pϭ0.030 for monocyte chemoattractant protein-1 by ANOVA). Combined therapyor losartan alone significantly increased plasma adiponectin levels and insulin sensitivity (determined by QUICKI)relative to baseline measurements. These changes were significantly greater than in the group treated with simvastatinalone (PϽ0.001 for adiponectin, Pϭ0.029 for QUICKI by ANOVA). Conclusions—Simvastatin combined with losartan improves endothelial function and reduces inflammatory markers to a
greater extent than monotherapy with either drug in hypercholesterolemic, hypertensive patients. (Circulation. 2004; 110:3687-3692.) Key Words: angiotensin Ⅲ endothelium Ⅲ hypercholesterolemia Ⅲ hypertension Ⅲ insulin
Hypercholesterolemia and hypertension are major public onset of new diabetes.1,4 The mechanisms of this benefit may
health problems that are frequently treated with statins
relate to the ability of these therapies to reduce insulin
and angiotensin II type 1 (AT1) receptor blockers, respec-
resistance.5 Moreover, it is possible that simvastatin com-
tively. Although the mechanisms of action for these 2 classes
bined with losartan therapy may have additional vascular
of drugs differ, both classes have beneficial effects on the
benefits that are greater than those observed for either drug
vasculature. Indeed, large-scale clinical studies have demon-
strated that simvastatin, an HMG-CoA reductase inhibitor,
Statins reduce LDL cholesterol. In addition, they improve
and losartan, an AT1 receptor blocker, prevent and retard the
endothelial function via stimulation of nitric oxide (NO)
progression of coronary heart disease.1,2 Hypertension and
synthase activity and mediate antioxidant effects that result in
coronary heart disease are frequently associated with insulin
enhanced NO bioactivity.6,7 AT1 receptor blockers also
resistance and disorders of metabolic homeostasis such as
improve endothelial function.8,9 This may be due in part to
obesity and type II diabetes. The endothelial dysfunction
diminished intracellular production of superoxide anions via
associated with cardiovascular diseases may contribute to
reduced activity of angiotensin II– dependent oxidases.10
insulin resistance and the pathophysiology of diabetes and its
Inhibition of the production of superoxide anions may limit
vascular complications.3 In fact, large-scale clinical studies
oxidation of LDL and contribute to increased NO bioactivity
have demonstrated that simvastatin and losartan reduce the
by limiting oxidative degradation of NO.7 Thus, AT1 receptor
Received June 5, 2004; revision received July 27, 2004; accepted July 27, 2004. From Cardiology (K.K.K., S.H.H., W.-J.C., T.H.A., I.S.C., E.K.S.), Laboratory Medicine (J.Y.A., Y.-H.S.), and Endocrinology (M.H.K.), Gachon
Medical School, Incheon, Korea, and Diabetes Unit, Laboratory of Clinical Investigation, NCCAM, NIH (M.J.Q.), Bethesda, Md.
Correspondence to Kwang Kon Koh, MD, PhD, FACC, FAHA, Professor of Medicine, Director, Vascular Medicine and Atherosclerosis Unit,
Cardiology, Gil Heart Center, Gachon Medical School, 1198 Kuwol-dong, Namdong-gu, Incheon, Korea. E-mail [email protected]
2004 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org DOI: 10.1161/01.CIR.0000143085.86697.13 3687 3688 Circulation December 14, 2004 Baseline Characteristics of the Study Population
frequently) during the study. Calcium channel or -adrenergicblockers were withheld for Ն48 hours before the study to avoid the
effects of these drugs. The Gil Hospital Institute Review Board
approved the study, and all participants gave written, informedconsent. Laboratory Assays
Blood samples for laboratory assays were obtained at approximately8 AM after patients fasted overnight before and at the end of each
2-month treatment period. These samples were immediately coded
so that investigators performing laboratory assays were blinded to
subject identity or study sequence. Assays for lipids, glucose, andplasma malondialdehyde (MDA), monocyte chemoattractant protein
BMI indicates body mass index. Values are expressed as meanϮSEM when
(MCP)-1, and adiponectin were performed in duplicate by ELISA
(BIOXYTECH LPO-586, OxisResearch, and R&D Systems, Inc)and assays for high-sensitivity C-reactive protein (hsCRP) levels by
latex agglutination [CRP-Latex(II), Denka-Seiken] as previously
described.7,8,18 Assays for plasma insulin levels were performed in
The endothelial dysfunction associated with diabetes, obe-
duplicate by immunoradiometric assay (INSULIN-RIABEAD II,Abbott Japan). The interassay and intra-assay coefficients of varia-
sity, metabolic syndrome, and other insulin-resistant states is
tion were Ͻ6%. Quantitative Insulin-Sensitivity Check Index
characterized by impaired NO release from endothelium.12
(QUICKI), a surrogate index of insulin sensitivity, was calculated as
Thus, improvement in endothelial function is predicted to
follows (insulin is expressed in U/mL and glucose in mg/dL):
enhance insulin sensitivity, and this may be a mechanism by
QUICKIϭ1/[log(insulin)ϩlog(glucose)].19
which simvastatin and losartan decrease the incidence of
Vascular Studies
new-onset diabetes. Adiponectin is one of a number of
Imaging studies of the right brachial artery were performed with an
proteins secreted by adipose cells that may couple regulation
ATL HDI 3000 ultrasound machine (Bothell) equipped with a
of insulin sensitivity with energy metabolism and serve to
10-MHz linear-array transducer based on a previously published
link obesity with insulin resistance.13 In humans, plasma
technique.7,8,18,20 Measurements were performed by 2 independent
levels of adiponectin are negatively correlated with adiposity,
investigators (S.H.H. and W.-J.C.) blinded to the subject’s identity
and decreased plasma adiponectin levels are observed in
and medication status. Measurements of maximum diameter andpercent flow-mediated dilation were made in 10 studies selected at
patients with diabetes and those with coronary artery dis-
random. The interobserver and intraobserver variabilities for re-
ease.14,15 Thus, decreased levels of adiponectin may play a
peated measurement of maximum diameter were 0.01Ϯ0.06 and
key role in the development of insulin resistance. In addition,
0.008Ϯ0.05 mm, respectively. The interobserver and intraobserver
adiponectin also possesses antiatherogenic properties.16,17
variabilities for repeated measurement of percent flow-mediated
Because the impact of simvastatin and losartan therapies
dilation were 0.12Ϯ1.31% and 0.10Ϯ1.29%, respectively.
on NO bioactivity and its subsequent effects on oxidant
Statistical Analysis
stress, inflammation, endothelial function, and insulin resis-
Data are expressed as meanϮ SEM or median (25% to 75% range).
tance may differ, we hypothesized that combined therapy
After testing data for normality, we used Student’s paired t or
may have additive beneficial effects that are greater than
Wilcoxon signed-rank test to compare values before and after each
those observed with either simvastatin or losartan therapy
treatment and the relative changes in values in response to treatment,
alone in hypercholesterolemic, hypertensive patients.
as reported in Tables 2 and 3. The effects of the 3 therapies onvascular function, markers of oxidant stress and inflammation, andinsulin sensitivity relative to baseline values were analyzed by 1-way
repeated-measures ANOVA or Friedman’s repeated ANOVA on
Study Population and Design
ranks. After demonstration of significant differences among thera-pies by ANOVA, post hoc comparisons between treatment pairs
Fifty hypercholesterolemic, hypertensive patients (LDL cholesterol
were made by use of the Student-Newman-Keuls multiple compar-
levels Ն100 mg/dL) participated in this study. We defined hyper-
ison procedures. Pearson’s correlation coefficient analysis was used
tension as systolic and diastolic blood pressure Ն140 or
to assess associations between measured parameters. We calculated
90 mm Hg, respectively. We excluded patients with severe hyper-
that 30 subjects would provide 80% power for detecting a difference
tension, unstable angina, or acute myocardial infarction. To mini-
of absolute increase, Ն2.1% flow-mediated dilation of the brachial
mize acute side effects to losartan, study medication was titrated
artery between baseline and simvastatin, with ␣ϭ0.05 based on our
from 50 to 100 mg upward over a 2-week period if no hypotension
previous studies.7,20 The comparison of endothelium-dependent di-
(systolic blood pressure Ͻ100 mm Hg) was noted. At the end of this
lation among the 3 treatment schemes was prospectively designated
time, participants were receiving either placebo or losartan 100 mg/d.
as the primary end point of the study. All other comparisons were
Of 50 patients, 47 tolerated losartan 100 mg with regard to
considered secondary. A value of PϽ0.05 was considered statisti-
maintaining systolic blood pressure Ͼ100 mm Hg for 3 hours after
drug administration and experienced no adverse effects from ther-apy. One patient was hypotensive, and the other 2 patients sufferedfrom dry cough. Thus, a total of 47 patients’ data were analyzed. The
clinical characteristics of these patients are summarized in Table 1.
When baseline values before each treatment period were
Patients were randomly assigned to one of the 3 treatments:
compared among the 3 treatment arms, no significant differ-
simvastatin 20 mg and placebo, simvastatin 20 mg and losartan 100
ences were noted in any of the parameters measured (Tables
mg, or losartan 100 mg and placebo daily during 2 months. This was
2 and 3). To rule out the possibility of a carryover effect from
a randomized, double-blind, placebo-controlled study with 3 treat-ment arms (each 2 months) and crossover with 2 washout periods
one treatment period to the next, we compared baseline
(each 2 months). The patients were seen at 14-day intervals (or more
values before the first treatment period to those before the
Simvastatin Combined With Losartan 3689 Effects of Simvastatin, Combined Therapy, and Losartan on Lipid Levels and Endothelial Function in Hypercholesterolemic, Hypertensive Patients
S indicates simvastatin; C, combined therapy; L, losartan; BP, blood pressure; Apo, apolipoprotein; and NTG, nitroglycerin. Data are expressed as meanϮSEM or
median (25th to 75th percentiles). There were no significant differences among each baseline value.
*PϽ0.05, †PϽ0.01, ‡PϽ0.001 vs each baseline value.
second and third treatment periods. There were no significant
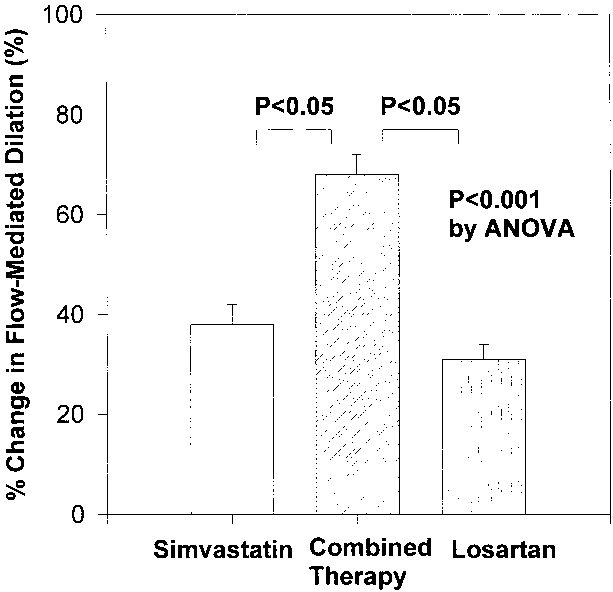
hyperemia relative to baseline measurements by 38Ϯ4%,
differences in any of the measured parameters in this analysis.
68Ϯ4%, and 31Ϯ3%, respectively (all PϽ0.001); however,combined therapy significantly improved this response more
Effects of Therapies on Blood Pressure and Lipids
than simvastatin or losartan alone (PϽ0.001 by ANOVA;
Losartan alone or combined therapy significantly reduced sys-
Figure 1 and Table 2). The brachial artery dilator response to
tolic and diastolic blood pressures after 2 months of administra-
nitroglycerin was similar for all therapies and was not
tion compared with baseline. These reductions were signifi-
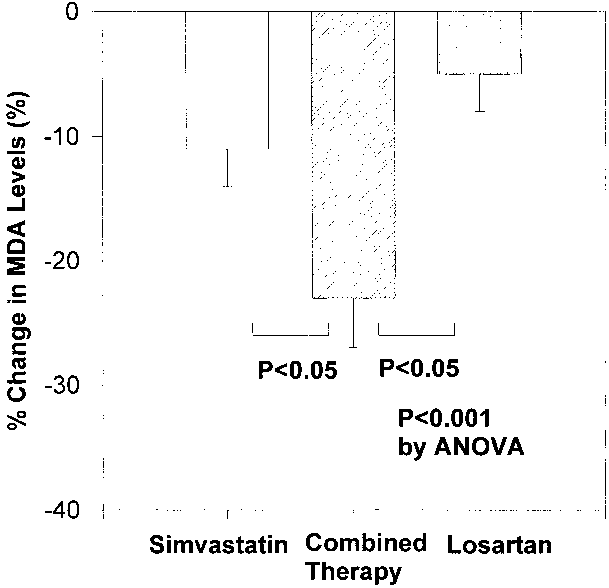
significantly changed from baseline values. Simvastatin,
cantly greater than that observed with simvastatin alone
combined therapy, and losartan significantly decreased the
(PϽ0.001 by ANOVA). Simvastatin alone or combined therapy
plasma MDA levels relative to baseline measurements by
significantly lowered total cholesterol (both PϽ0.001), LDL
11Ϯ3% (PϽ0.001), 23Ϯ4% (PϽ0.001), and 5Ϯ3%
cholesterol (both PϽ0.001), and apolipoprotein B levels (both
(Pϭ0.040), respectively; however, combined therapy signif-
PϽ0.001) compared with baseline. These reductions were sig-
icantly reduced MDA levels more than simvastatin or losar-
nificantly greater than those observed with losartan alone(PϽ0.001 by ANOVA). However, there were no significant
tan alone (PϽ0.001 by ANOVA; Figure 2 and Table 2).
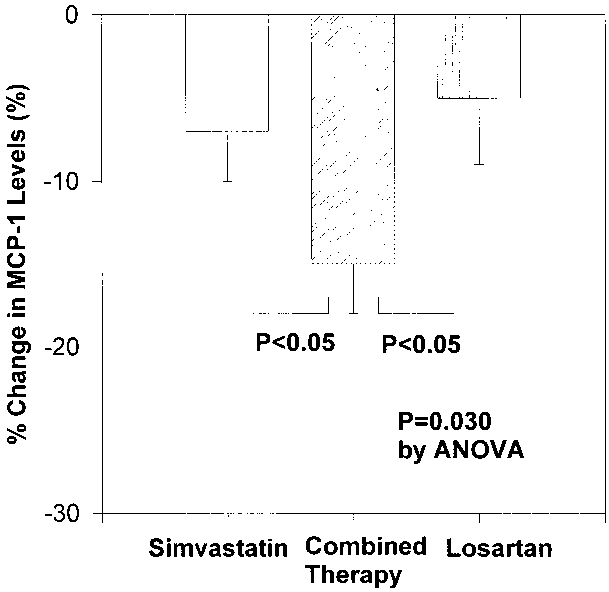
differences between simvastatin alone and combined therapy forthese parameters (Table 2). Effects of Therapies on Markers of Inflammation Simvastatin, combined therapy, and losartan significantly Effects of Therapies on Vasomotor Function
decreased plasma MCP-1 levels relative to baseline measure-
ments by 7Ϯ3% (Pϭ0.003), 15Ϯ3% (PϽ0.001), and 5Ϯ4%
Simvastatin, combined therapy, and losartan significantly
(Pϭ0.048), respectively, however, combined therapy signif-
improved the percent flow-mediated dilator response to
icantly decreased MCP-1 levels more than simvastatin or
Effects of Simvastatin, Combined Therapy, and Losartan on Adiponectin Levels and Insulin Resistance in Hypercholesterolemic, Hypertensive Patients
S indicates simvastatin; C, combined therapy; L, losartan; and ADP, adiponectin. Data are expressed as meanϮSEM or median (25th to 75th percentiles). There
were no significant differences among each baseline value. 3690 Circulation December 14, 2004 Figure 1. Percent change in flow-mediated dilation from pre- Figure 3. Percent change in MCP-1 levels from pretreatment
treatment values after treatment with simvastatin alone, com-
values after treatment with simvastatin alone, combined therapy,
bined therapy, and losartan alone (PϽ0.001 by ANOVA). Bars
and losartan alone (Pϭ0.030 by ANOVA). Bars identify SEM.
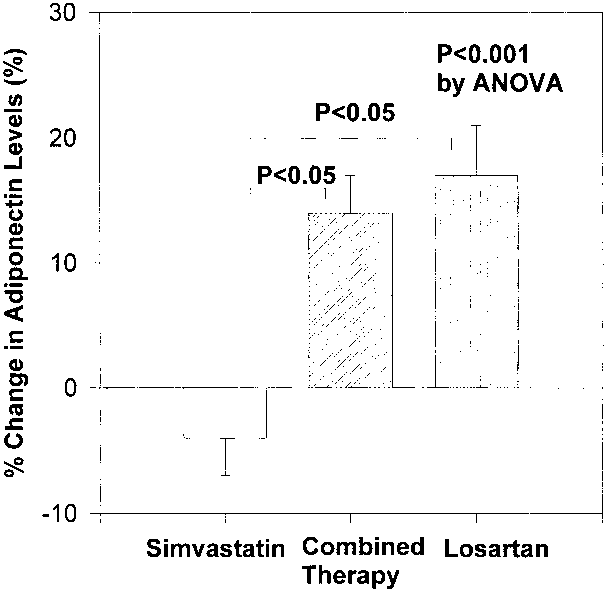
to 5.27 (Pϭ0.002), respectively. These increases were signif-
losartan alone (Pϭ0.030 by ANOVA; Figure 3 and Table 2).
icantly greater than those observed with simvastatin alone
Simvastatin, combined therapy, and losartan significantly
(PϽ0.001 by ANOVA; Figure 4 and Table 3). The 3
lowered plasma hsCRP levels relative to baseline measure-
therapies did not have significantly different baseline insulin
ments from 0.85 to 0.80 mg/L (Pϭ0.042), 0.85 to 0.65 mg/L
and glucose levels. However, the magnitude of reduction of
(Pϭ0.002), and 0.85 to 0.80 mg/L (Pϭ0.042), respectively;
insulin with combined therapy or losartan alone was signifi-
however, the magnitude of reduction among these 3 therapies
cantly greater than with simvastatin alone (Pϭ0.041 by
was not statistically significant (Pϭ0.146 by ANOVA).
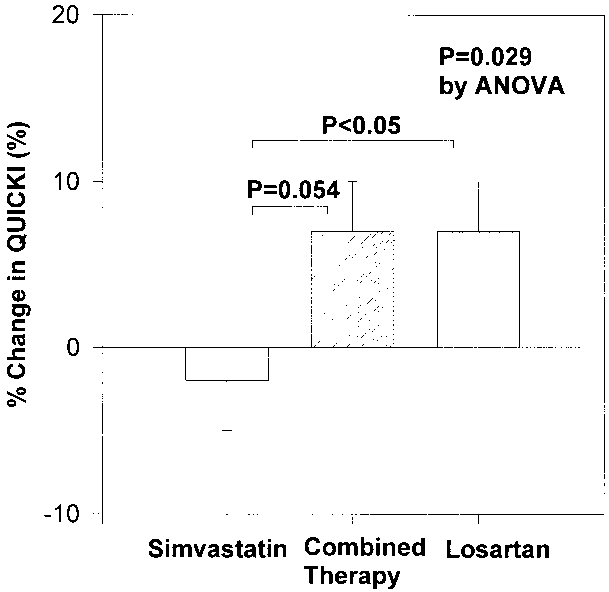
ANOVA; Table 3). Combined therapy or losartan alone
Effects of Therapies on Adiponectin and
significantly increased QUICKI relative to baseline measure-
Insulin Resistance
ments by 7Ϯ3% (Pϭ0.032) and 7Ϯ3% (Pϭ0.042), respec-
There were significant inverse correlations between body
tively. These increases were significantly greater than those
observed with simvastatin alone (Pϭ0.029 by ANOVA;
(rϭϪ0.332, Pϭ0.023 before simvastatin; rϭϪ0.328,
Figure 5 and Table 3). There were correlations between
Pϭ0.024 before combined therapy; rϭϪ0.292, Pϭ0.046
percent changes in adiponectin levels and percent changes in
before losartan). There were significant inverse correlations
QUICKI (rϭ0.245, Pϭ0.097 after simvastatin; rϭ0.316,
between baseline adiponectin levels and baseline triglyceride
Pϭ0.030 after combined therapy; rϭ0.433, Pϭ0.002 after
levels (rϭϪ0.351, Pϭ0.016 before simvastatin; rϭϪ0.325,
losartan). There were inverse correlations between percent
Pϭ0.026 before combined therapy; rϭϪ0.342, Pϭ0.019
changes in adiponectin levels and percent changes in insulin
before losartan). There were significant correlations between
(rϭϪ0.171, Pϭ0.251 after simvastatin; rϭϪ0.352, Pϭ0.015
baseline adiponectin levels and baseline HDL cholesterol
after combined therapy; rϭϪ0.367, Pϭ0.011 after losartan).
levels (rϭ0.401, Pϭ0.005 before simvastatin; rϭ0.399,
We investigated whether losartan-induced changes in the
Pϭ0.006 before combined therapy; rϭ0.303, Pϭ0.039 be-
percent flow-mediated dilator response to hyperemia, sero-
fore losartan). Combined therapy and losartan alone signifi-
logical markers of oxidant stress and inflammation, and
cantly increased the plasma adiponectin levels relative to
insulin resistance were mediated by a reduction in systolic or
baseline measurements from 4.63 to 5.02 (PϽ0.001) and 4.19
Figure 4. Percent change in adiponectin levels from pretreat- Figure 2. Percent change in MDA levels from pretreatment val-
ment values after treatment with simvastatin alone, combined
ues after treatment with simvastatin alone, combined therapy,
therapy, and losartan alone (PϽ0.001 by ANOVA). Bars iden-
and losartan alone (PϽ0.001 by ANOVA). Bars identify SEM. Simvastatin Combined With Losartan 3691
apy in the present study are consistent with experimental andclinical studies.21,28
Losartan therapy alone resulted in significant elevation of
adiponectin levels, decreased insulin levels, and increasedinsulin sensitivity (assessed by QUICKI). The present studyis the first report demonstrating that losartan therapy canincrease adiponectin levels. Adiponectin is an adipose-derived factor that augments and mimics metabolic actions ofinsulin. Increasing adiponectin levels would be predicted toimprove both insulin sensitivity and endothelial function bymultiple mechanisms. Regulation of metabolic homeostasisand hemodynamic homeostasis may be coupled by vascularactions of insulin to stimulate production of NO.16 Thus,
Figure 5. Percent change in QUICKI from pretreatment values
improvements in endothelial function may increase insulin
after treatment with simvastatin alone, combined therapy, and
sensitivity, whereas increased insulin sensitivity may improve
losartan alone (Pϭ0.029 by ANOVA). Bars identify SEM.
endothelial function.12 Interestingly, in contrast to the effectsof combination therapy on flow-mediated dilation, MDA,
diastolic blood pressure. There were no significant correla-
CRP, and MCP-1, the beneficial effects of losartan therapy on
tions between these changes and reduction of systolic blood
adiponectin levels, insulin levels, and insulin sensitivity did
pressure (Ϫ0.134ՅrՅ0.077) or between these changes and
not increase further with combination therapy. This finding
reduction of diastolic blood pressure (Ϫ0.295ՅrՅ0.172).
suggests that improving endothelial function per se (as
After combined therapy, improvement in flow-mediated di-
reflected by flow-mediated dilation) may not completely
lation correlated with changes in MDA levels (rϭϪ0.422 and
explain the effects of losartan or combined therapy to
Pϭ0.003), MCP-1 levels (rϭ0.189 and Pϭ0.204), hsCRP
improve insulin sensitivity. In other words, there may be
(rϭϪ0.137 and Pϭ0.357), adiponectin levels
additional mechanisms for losartan or combined therapy to
(rϭ0.420 and Pϭ0.003), QUICKI (rϭ0.258 and Pϭ0.080),
improve insulin sensitivity that are independent of endothelial
and insulin levels (rϭϪ0.251 and Pϭ0.089).
function, eg, direct effects of losartan on glucose insulin–stimulated glucose uptake or promotion of adipogenic differ-
Discussion
entiation of preadipocytes29 or induction of peroxisome pro-
In our hypercholesterolemic, hypertensive cohort, simvastatin
therapy alone significantly improved the lipid profile,
differentiation in adipocytes.30 Effects of losartan or com-
whereas losartan therapy alone significantly lowered blood
bined therapy to increase adiponectin levels may in part
pressure as expected. Comparable beneficial effects on both
mediate improved insulin sensitivity, which is supported by
lipids and blood pressure were observed with combination
the significant correlation shown in the present study. On the
therapy. We reasoned that distinct biological actions of
other hand, combined therapy may reduce insulin resistance
simvastatin and losartan therapies on lipoproteins and the
by multiple mechanisms such as lipoprotein changes and
angiotensin system may improve endothelium-dependent
reduced oxidant stress that also contribute to NO bioavail-
vascular function by different mechanisms. Indeed, although
ability. The effects of losartan or combined therapy on
monotherapy with simvastatin or losartan significantly im-
flow-mediated dilation, oxidant stress and inflammation
proved endothelial function and inflammatory markers (as-
markers, and insulin resistance were independent of blood
sessed by flow-mediated dilation, MDA levels, CRP levels,
pressure changes and consistent with recent randomized
and MCP-1 levels), combined therapy had additional substan-
clinical trials.2,31 Likewise, several studies suggest a hypoth-
tial and significant beneficial effects on these parameters over
esis that the effects of AT1 receptor blockers to improve
those seen with monotherapy for either drug, which may
endothelial function are due to other factors in addition to a
explain the observations of a recent clinical trial.21
The additional beneficial effects of combined simvastatin/
Metabolic syndrome is associated with atherosclerotic
losartan therapy may be the result of several interacting
disease. Patients with metabolic syndrome make up one of the
mechanisms. For example, angiotensin II is very potent
largest groups of individuals with both hyperlipidemia and
endogenous vasoconstrictor, whereas LDL induces upregula-
hypertension. Obesity is one of the most common causes of
tion of the AT1 receptor.22 Indeed, hypercholesterolemic
cardiovascular disease. In the present study, more than half of
rabbits display enhanced vascular expression of AT1 recep-
the subjects were overweight. We observed that plasma levels
tors that mediate increased activity of angiotensin II.23 Fur-
of adiponectin were significantly inversely correlated with
thermore, the effect of statins to reverse the elevated blood
body mass index. We also observed significant correlations
pressure response to angiotensin II infusion is accompanied
between baseline adiponectin levels and baseline HDL cho-
by downregulated AT1 receptor density.24,25 Angiotensin II
lesterol or triglyceride levels. Thus, our study may have
promotes superoxide anion generation and endothelial dys-
implications for the treatment of patients with metabolic
function.8,26 CRP upregulates AT1 receptors in vascular
smooth muscle cells, and these effects are attenuated by
In summary, our study suggests that combination therapy
losartan.27 The additive beneficial effects of combined ther-
with simvastatin and losartan has beneficial additive effects
3692 Circulation December 14, 2004
on endothelial function and inflammatory markers. This may
coronary artery disease in men. Arterioscler Thromb Vasc Biol. 2003;23:
be due to combined effects of the respective monotherapies to
15. Yu JG, Javorschi S, Hevener AL, et al. The effect of thiazolidinediones
improve lipid profile, blood pressure, adiponectin levels, and
on plasma adiponectin levels in normal, obese, and type 2 diabetic
insulin sensitivity. The additive beneficial effects of com-
subjects. Diabetes. 2002;51:2968 –2974.
bined therapy are predicted to reduce cardiovascular events in
16. Chen H, Montagnani M, Funahashi T, et al. Adiponectin stimulates
production of nitric oxide in vascular endothelial cells. J Biol Chem.
hypercholesterolemic, hypertensive patients more than mono-
17. Ouchi N, Kihara S, Arita Y, et al. Adipocyte-derived plasma protein,
adiponectin, suppresses lipid accumulation and class A scavenger
Acknowledgments
receptor expression in human monocyte-derived macrophages. Circu-lation. 2001;103:1057–1063.
This study was supported in part by grants from the Korea Society of
18. Koh KK, Jin DK, Yang SH, et al. Vascular effects of synthetic or natural
Hypertension (KSH-2004). We express our gratitude to Han Gyu
progestagen combined with conjugated equine estrogen in healthy post-
Kim, MT, Sang Kyoon Kwon, MT, Jeong Bum Park, MT, Hyo Ju
menopausal women. Circulation. 2001;103:1961–1966.
Park, BA, and Soo Jin Kim, RN, for their excellent technical
19. Katz A, Nambi SS, Mather K, et al. Quantitative insulin sensitivity check
index: a simple, accurate method for assessing insulin sensitivity inhumans. J Clin Endocrinol Metab. 2000;85:2402–2410. References
20. Koh KK, Son JW, Ahn JY, et al. Comparative effects of diet and statin on
nitric oxide bioactivity and matrix metalloproteinases in hypercholester-
1. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection
olemic patients with coronary artery disease. Arterioscler Thromb Vasc
Study of cholesterol lowering with simvastatin in 20,536 high-risk indi-
viduals: a randomised placebo-controlled trial. Lancet. 2002;360:7–22.
21. Sever PS, Dahlof B, Poulter NR, et al, for the ASCOT Investigators.
2. Dahlof B, Devereux RB, Kjeldsen SE, et al, for the LIFE Study Group.
Prevention of coronary and stroke events with atorvastatin in hyper-
Cardiovascular morbidity and mortality in the Losartan Intervention For
tensive patients who have average or lower-than-average cholesterol
Endpoint Reduction in Hypertension Study (LIFE): a randomised trial
concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial–Lipid
against atenolol. Lancet. 2002;359:995–1003.
Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial.
3. Creager MA, Luscher TF, Cosentino F, et al. Diabetes and vascular
Lancet. 2003;361:1149 –1158.
disease: pathophysiology, clinical consequences, and medical therapy,
22. Nickenig G, Sachinidis A, Michaelsen F, et al. Upregulation of vascular
part I. Circulation. 2003;108:1527–1532.
angiotensin II receptor gene expression by low-density lipoprotein in
4. Lindholm LH, Ibsen H, Borch-Johnsen K, et al, for the LIFE Study
vascular smooth muscle cells. Circulation. 1997;95:473– 478.
Group. Risk of new-onset diabetes in the Losartan Intervention For
23. Nickenig G, Jung O, Strehlow K, et al. Hypercholesterolemia is asso-
Endpoint Reduction in Hypertension Study. J Hypertens. 2002;20:
ciated with enhanced angiotensin AT1-receptor expression. Am J Physiol.
5. Folli F, Kahn CR, Hansen H, et al. Angiotensin II inhibits insulin
24. Nickenig G, Baumer AT, Temur Y, et al. Statin-sensitive dysregulated
signaling in aortic smooth muscle cells at multiple levels: a potential role
AT1 receptor function and density in hypercholesterolemic men. Circu-
for serine phosphorylation in insulin/angiotensin II crosstalk. J Clinlation. 1999;100:2131–2134. Invest. 1997;100:2158 –2169.
25. Dechend R, Fiebeler A, Park JK, et al. Amelioration of angiotensin
6. Koh KK. Effects of statins on vascular wall: vasomotor function, inflam-
II–induced cardiac injury by a 3-hydroxy-3-methylglutaryl coenzyme a
mation, and plaque stability. Cardiovasc Res. 2000;47:648 – 657.
reductase inhibitor. Circulation. 2001;104:576 –581.
7. Koh KK, Cardillo C, Bui MN, et al. Vascular effects of estrogen and
26. Fukai T, Siegfried MR, Ushio-Fukai M, et al. Modulation of extracellular
cholesterol-lowering therapies in hypercholesterolemic postmenopausal
superoxide dismutase expression by angiotensin II and hypertension. Circ
women. Circulation. 1999;99:354 –360.
8. Koh KK, Ahn JY, Han SH, et al. Pleiotropic effects of angiotensin II
27. Wang CH, Li SH, Weisel RD, et al. C-reactive protein upregulates
receptor blocker in hypertensive patients. J Am Coll Cardiol. 2003;42:
angiotensin type 1 receptors in vascular smooth muscle. Circulation.
9. Prasad A, Tupas-Habib T, Schenke WH, et al. Acute and chronic angio-
28. Delbosc S, Cristol JP, Descomps B, et al. Simvastatin prevents angioten-
tensin-1 receptor antagonism reverses endothelial dysfunction in athero-
sin II–induced cardiac alteration and oxidative stress. Hypertension.
sclerosis. Circulation. 2000;101:2349 –2354.
10. Griendling KK, Minieri CA, Ollerenshaw JD, et al. Angiotensin II stim-
29. Sharma AM, Janke J, Gorzelniak K, et al. Angiotensin blockade prevents
ulates NADH and NADPH oxidase activity in cultured vascular smooth
type 2 diabetes by formation of fat cells. Hypertension. 2002;40:
muscle cells. Circ Res. 1994;74:1141–1148.
11. Hayek T, Attias J, Coleman R, et al. The angiotensin-converting enzyme
30. Schupp M, Janke J, Clasen R, et al. Angiotensin type 1 receptor blockers
inhibitor, fosinopril, and the angiotensin II receptor antagonist, losartan,
induce peroxisome proliferator–activated receptor-␥ activity. Circulation.
inhibit LDL oxidation and attenuate atherosclerosis independent of
lowering blood pressure in apolipoprotein E deficient mice. Cardiovasc
31. Sleight P, Yusuf S, Pogue J, et al, for the Heart Outcomes Prevention
Evaluation (HOPE) Study. Blood-pressure reduction and cardiovascular
12. Vincent MA, Montagnani M, Quon MJ. Molecular and physiologic
risk in HOPE Study. Lancet. 2001;358:2130 –2131.
actions of insulin related to production of nitric oxide in vascular endo-
32. Schiffrin EL, Park JB, Intengan HD, et al. Correction of arterial structure
thelium. Curr Diab Rep. 2003;3:279 –288.
and endothelial dysfunction in human essential hypertension by the an-
13. Heilbronn LK, Smith SR, Ravussin E. The insulin-sensitizing role of the
giotensin receptor antagonist losartan. Circulation. 2000;101:1653–1659.
fat derived hormone adiponectin. Curr Pharm Des. 2003;9:1411–1418.
33. Wassmann S, Hilgers S, Laufs U, et al. Angiotensin II type 1 receptor
14. Kumada M, Kihara S, Sumitsuji S, et al, for the Osaka CAD Study Group.
antagonism improves hypercholesterolemia-associated endothelial dys-
Coronary artery disease: association of hypoadiponectinemia with
function. Arterioscler Thromb Vasc Biol. 2002;22:1208 –1212.
I.5.2.1.14. Ingresos por Actos de Coordinación derivados del Acuerdo de Colaboración Administrativa, por la Participación de la Recaudación del Impuesto sobre Automóviles Nuevos En el apartado II.1, “Política de Ingresos”, de la Cuenta Pública del Gobierno del Distrito Federal de 2007, se señala que por concepto de Ingresos por Actos de Coordinación Derivados del Acuerdo
Inhaled QUICK RELIEF Medications Generic Name Brand Name Strengths (# Doses/Inhaler) Comments Short-Acting Beta2-Agonists Pre-mixed unit dose (3 mL); vials must be placed back in the foil wrap after the foil wrap is opening; expires 1 week after foil wrap is opened Albuterol for Nebulization 0.25-0.5 mL can be added to 2-3 mL saline Supplied as 20 mL droppe
 Additive Beneficial Effects of Losartan Combined With
Additive Beneficial Effects of Losartan Combined With 3688
3688 Simvastatin Combined With Losartan
Simvastatin Combined With Losartan
 3690
3690
 Simvastatin Combined With Losartan
Simvastatin Combined With Losartan 3692
3692