MEDEX Porter Mortality Project 2010 EXPEDITION HEALTH PREPARATION AND IMMUNISATION ADVICE MEDEX RESEARCH EXPEDITION 2010
IMMUNISATIONS should be discussed with your own doctor or practice nurse for the most up to
date guidelines. Vaccinations are also available from commercial centres such as British Airways
travel clinics. Remember that a course can take several weeks so book in early. This information is
not exhaustive but all of the following should be carefully considered:
Essential routine UK Vaccinations – please ensure that these are up to date: Polio (L) Tetanus is contracted through dirty cuts and scratches and poliomyelitis spread
through contaminated food and water. They are serious infections of the nervous
Diphtheria
system. UK advice is for lifetime total of 5 tetanus shots unless at particular risk of soil-
contaminated wounds such as farmers. 10 yearly boosters advised for travelers to
countries with poor access to post-exposure tetanus immunoglobulin.
Additional essential recommendations for Nepal: Typhoid and hepatitis A are spread through contaminated food and water. Typhoid
causes septicaemia and hepatitis A causes liver inflammation and jaundice. A single
Hepatitis A
dose of inactivated Hepatitis A vaccine is effective and recommended, with a booster at
12 months for life-long immunity. Typhoid vaccine requires a booster every 3 years.
NB: Climber with typhoid evacuated from Medex Kangchenjunga expedition in 1998!
Rabies is endemic in Nepal and is spread through bites or licks on broken skin from
infected animals. It is always fatal without post-exposure treatment. Vaccination is
advised since we wil be very remote from any reliable source of vaccine. Even when
pre-exposure vaccines have been received urgent medical advice should be sought
after any animal bite. Strongly recommended to have 3-dose course (day 0, 7, 28)
intramuscularly. Those with 2-dose course, or given intradermal y,or whose last vaccine
>2 years ago, are incompletely immunised and wil require further vaccines plus
immunoglobulin which may be difficult to obtain in Nepal. Completely immunised
individuals need only 2 doses of post bite vaccine and have more time to obtain it.
Injections whilst taking chloroquine/mefloquine may be less effective. Boost at 2 years.
Tuberculosis is most commonly transmitted via droplet infection. Endemic in Nepal with
increased risk if in contact with locals. Dept. of Health recommends if >1 month in Asia.
Re-immunisation for those who received standard UK single BCG is not required.
Meningitis Meningococcal meningitis is spread through close personal contact. Vaccination is
recommended. Risk mostly Group A strain so ensure Meningococcal AC vaccine.
Hepatitis B Hepatitis B is spread through infected blood, contaminated needles and sexual
intercourse, It affects the liver, causing jaundice and occasional y liver failure. Carriage
in the local population said to be high (>10%). Vaccination recommended for health care
workers, those who may be handling blood or bodily fluids. Those previously immunised
MEDEX Porter Mortality Project 2010 To be considered: Japanese B Japanese B encephalitis is spread by mosquitoes. It is a serious infection of the brain Encephalitis
and vaccination is advised for those in risk areas unable to avoid mosquito bites, staying
for long periods (e.g. more than 4 weeks) or visiting rural areas. Two doses 1-2 wks
NB. December 2005, nearly 3000 cases of Japanese encephalitis were reported of which >300 people died.
The most affected areas were in the western, mid-western and far-western regions of Nepal.
For further details of areas affected please see the WHO Regional Office for S.E. Asia website.
Influenza and
For those at risk of serious disease or complications e.g. those with heart/chest disease
Pneumoccocus or chronic il ness such as diabetes.
Measles, Mumps, Rubel a – in those not previously infected or immunised.
Yellow Fever
Is not required for Nepal, BUT vaccination with certificate is required if arriving from or
through an infected country (neither India nor China is considered an infected zone).
No malarial prophylaxis is required in Kathmandu or areas over 1300m. Most malaria transmission
in Nepal is in the low lying southern plains or 'terrai' districts of Bara, Dhanukha, Kapilvastu,
Mahotari, Parsa, Rautahat, Rupendehi and Sarlahi. Risk here is low but there are anecdotal reports
of altitude climbers contracting malaria when being evacuated by helicopters which have put down
If you are planning to travel to areas below 1300m for any substantial time period then mosquito bite
avoidance and malaria tablets are advised. Current recommendations are:
Chloroquine 300mg weekly (2x 150mg tablets supplied as Nivaquine or Avloclor)
PLUS Proguanil 200mg daily (2x 100mg tablets, Paludrine)
If you are planning on visiting malarial areas before or after the expedition please remember to start
tablets at least 1 week before exposure, continue the whole time in the risk area and for 4 weeks
after leaving. A different regime and drug may be required if you are travelling to another malaria
area before or after Nepal – please consult you travel clinic/GP. It is important to note that the
tablets don’t prevent malaria but interfere with its life cycle once inside the body. The only real
Bite Avoidance: Malaria mosquitoes bite mostly from dusk to dawn and like the thin skin of ankles
and wrists. Avoid mosquito bites by covering up with long sleeves and trousers especially after
sunset, using insect repellents (DEET is most effective) on exposed skin and, when necessary,
MEDEX Porter Mortality Project 2010
sleeping under an insecticide impregnated mosquito net. For a discussion from the CIWEC Travel
Clinic in Kathmandu, please see http://www.ciwec-clinic.com/immune/malaria.html
**If you have been traveling in a malarial area and develop a fever, seek medical attention promptly. Remember malaria can develop even up to one year after exposure** Other health considerations
Medical treatment is expensive at Western clinics in Nepal. Healthcare is poor in most areas outside
Kathmandu valley and Pokhara. You should be aware that it may be difficult to obtain rapid
helicopter evacuation if you were to fall il or suffer a serious accident in a remote area.
In the 2006 Report on the Global AIDS Epidemic the UNAIDS/WHO Working Group estimated that
around 74,000 adults aged 15 years or over in Nepal were living with HIV; the prevalence rate was
estimated at around 0.5% of the adult population. This compares to the prevalence rate in adults in
the UK of around 0.2%. You should exercise normal precautions to avoid exposure to HIV/AIDS.
Useful health information including infectious and non-infectious diseases, vaccinations, and travel
safety advice can be obtained from the National Travel Health Network and Centre website at
This site has excel ent advice sheets regarding common
expedition and altitude related il nesses and their treatment, camp hygiene, water purification,
travelers’ diarrhoea etc. These can be downloaded and printed.
Personal Medical Kit
You should take along a basic medical kit.
If you are planning to trek any length of time, remember that you wil enjoy the experience more if
you have done some fitness training ahead of time and tested out your boots!
Please visit in good time before the expedition. Toothache quickly spoils any trip and there is a limit
to dental procedures that can be performed in the field. Most of us don’t fancy having teeth out in
the safety of a dental surgery – it is highly unlikely that the idea wil seem any more palatable in
Insurance
This is mandatory and must cover any climbing, rafting or other activities in which you intend to
partake whilst in Nepal. Cover must include medical eventualities, search and rescue, and air
ambulance repatriation to your country of residence. Average travelers insurance may not cover you
for all your planned activities and including search and rescue is essential in case you need to be
Check the UK Foreign Office Website regularly for updates regarding the political situation in Nepal
The wealth of information on this site also includes details regarding visas for UK citizens and
Further queries
If you have any general or specific medical queries or concerns, please feel free to contact me and I
Dr Simon Currin
BRYGGEKLINIKKEN AS D o c S i d e - august 2009H1N1 (New Influenza)- also known as ”swine flu”The name “swine flu” is both stigmatising and misleading. As a result the Norwegian healthauthorities (and WHO) has now designated the condition as “new flu”. This is supported byus here at Bryggeklinikken, and we furthermore support the guidelines published by theNorwegian health authoriti
Events of increased particle number concentrations around trade wind cumuli near Barbados B. Wehner1, F. Ditas1, A. Wiedensohler1 and H. Siebert1 1Leibniz Institute for Tropospheric Research (TROPOS), 04318 Leipzig, Germany Keywords: new particle formation, clouds, ultrafine particles. Presenting author email: [email protected] Beside numerous measurements at ground-based stations, new par
 MEDEX Porter Mortality Project 2010
MEDEX Porter Mortality Project 2010 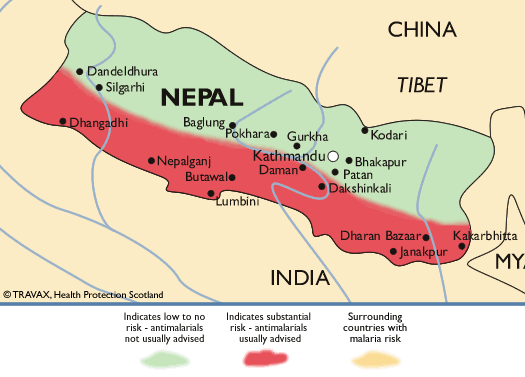 MEDEX Porter Mortality Project 2010
MEDEX Porter Mortality Project 2010