Clinical experience with a new implant in a minimally invasive procedure
Bilateral sinus floor elevation and simultaneous implantation In the following article, the author describes his clinical experience with a new implant that allows for augmentation of the maxillary sinus floor by hydraulic elevation of the Schneiderian membrane.
When dental implants are required in the maxillary
molar region, a sinus floor augmentation procedure
is indicated in 50 per cent or more of cases [1] due to
pneumatization of the maxillary sinus and atrophy of
the alveolar ridge [2]. The common procedure in mostcases is the open sinus lift, first presented by Boyneand James [3] and subsequently by Tatum [4].
However, the open sinus elevation involves com-
plications [5-9], significant trauma to the patientand usually a long recovery time involving pain,swelling and bleeding in the facial area, resulting inthe loss of a number of work days [10]. A commoncomplication is the perforation of the Schneiderianmembrane [2,8,9].
A relatively new alternative for safely elevating
the Schneiderian membrane is the hydraulic sinus
no connection between the prosthetic interface and
elevation, or hydraulic sinus condensing [11,12]: After
the duct, so bacteria from the oral cavity are blocked
careful drilling into the sinus floor without damag-
from reaching the bone after implantation.
ing the mucosa, the operator uses a liquid (Chen [11]uses an air/water aerosol emitted from a dental tur-
Case studies
bine) to create a hydraulic pressure that detachesthe Schneiderian membrane from the floor of the
This article describes two cases of bilateral sinus
sinus and forms a space under it. Bone substitute is
floor elevation, for a total of four sinus floor aug-
inserted into the resulting space, followed by a den-
mentation procedures. All four procedures were car-
tal implant. Hydraulic elevation is a safer method for
ried out in a similar manner. Two of the procedures
detaching the membrane, as the pressure is evenly
are described below in detail – one for each patient.
spread over the membrane surface [13].
The cases presented here used a new dental im -
First patient
plant (iRaise, Maxillent, Israel). This implant applies
The first patient was a 64-year-old woman who took
the principle of hydraulic elevation using an internal
metamizole for thyroid dysfunction but was other-
channel within the implant, which allows for the
wise healthy. Clinical and radiological examination
injection of saline to accomplish the membrane ele-
showed teeth 16, 17, 26 and 27 to be missing in the
vation. Thereafter, the saline is removed and a bone
region of the maxillary sinuses. The residual bone
graft with a gel-like consistency is inserted into the
height on both sides was up to 4 mm, requiring
newly formed sub-Schneiderian space; finally, the
bilateral sinus floor elevation as a prerequisite for
implant is fully inserted into the bone. The L-shaped
an implant-supported restoration. The two sinuses
internal channel (Fig. 1) is designed so that there is
appeared to be normal in a CT scan. Sinus floor
elevation and simultaneous implant insertion at
was raised by crestal incision, without release inci-
site 16 and another conventional implant insertion
sions. An osteotomy was prepared at site 26, and the
at site 17 were carried out, and sinus floor elevation
sinus floor was identified using a flat bur that pro-
and simultaneous implant insertion were per-
vides for tactile sensation of the hard cortical bone
formed at sites 26 (sinus lift implant) and 27 (con-
of the sinus floor, without any risk of rupture. After
ventional implant). The method provides for aug-
widening the bore, the sinus floor was weakened
mentation of a whole sinus using a single implant. If
using a specialized diamond bur. At this stage the
additional implants are required in the treated sinus,
implant was inserted into the bore. A tube connec-
conventional implants of any manufacture may be
tor was attached to the implant to enable the injec-
placed within the elevated space that already con-
tains bone graft material. In the cases described
The membrane was elevated by hydrostatic pres-
here, the conventional implants were iSure implants
sure by injecting 3 cm3 of normal saline solution
through the implant. The saline was removed from
Before treatment, the patient received prophy-
the sinus by withdrawing the syringe plunger and
lactic antibiotics (amoxicillin and clavulanic acid,
appeared to be mixed with a little blood (Fig. 4), a
875 mg) and performed a mouthwash (chlorhexidine
clinical indicator for the saline having come in con-
gluconate 0.12 %). A full-thickness mucoperiosteal flap
tact with the Schneiderian membrane, breachingthe small blood vessels between the membrane andthe sinus floor. Next, 3 cm3 of synthetic bone substi-tute were inserted (MBCP Gel, Biomatlante, France)(Fig. 5), selected because it is easily injected throughthe implant and is fairly radiopaque, allowing it tobe identified on post-operative X-rays.
The connector was removed and the implant fully
inserted into the bone. Beside the sinus lift implantat site 27, a conventional implant was placed usinga standard drilling protocol. This osteotomy wasdrilled directly into the sinus, inside the bone graftbeneath the elevated membrane. Figures 6 and 7
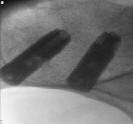
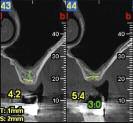
Figs. 6 and 7 CT scan before the treatment, periapical X-ray image after the treat-ment. iRaise is the left implant in the images.
show X-ray images before and after the treatment. Figs. 8 and 9Verification ofreaching thesinus floor byperiapical X-rayimage with adepth gauge.Second patient
The second patient was a 56-year-old man who had
had bypass surgery and took low-dose aspirin pro-
phylactically. Clinical and radiological examination
showed teeth 16, 17, 26 and 27 to be missing, with
approximately 4 mm of residual bone height bilater-
ally. The sinuses appeared normal in the CT scan. On
the right side, sinus floor elevation was performed
using the sinus lift implant at site 17. An additionalconventional implant was inserted at site 16. Onthe left side, the elevation and implantation wereperformed at site 27, and an additional conventionalimplant was inserted at site 26. On both sides, the
touched the Schneiderian membrane, detaching the
sinus lift implants were positioned in the distal loca-
blood vessels at its bottom (Fig. 10). A connector was
tions, due to the flat angulation of sinus floor, as
attached to the implant, and the membrane was ele-
opposed to a more angulated anatomy at sites 16
vated by hydrostatic pressure through injected saline.
The saline was drawn and fluid bone graft was insert-
The procedure on the left side is described in the
ed using three 1 cm3 syringes (Figs. 11 and 12).
following. The patient received antibiotic prophy-
Finally, the connector was removed from the
laxis before the treatment (amoxicillin and clavu-
implant and the implant was fully inserted into the
lanic acid, 875 mg). A flap was raised by crestal inci-
osteotomy. An additional conventional implant was
sion at sites 26 and 27, and preparatory osteotomies
inserted at site 26. Figures 13 and 14 show a CT image
were performed until the identification of the hard
before the treatment and a periapical X-ray image
bone of the sinus floor using a flat bur. The position
immediately after it. Figures 15 and 16 show the situ-
of the osteotomy with respect to the sinus floor was
ation at the follow-up at four and at seven months.
confirmed by periapical X-ray image with a depth
All four procedures were performed similarly to the
two cases described here in detail. Pre- and post-oper-
After widening the bore and weakening the sinus
ative X-ray images are provided for the two remain-
floor using a diamond bur, the implant was inserted.
ing cases (Figs. 17 to 22). Both patients immediately
Blood was identified at the lateral opening of the
resumed full activity and did not report any pain,
implant, indicating that the end of the implant had
Figs. 11 and 12Insertion of 3 cm3of bone graftthrough theimplant.Figs. 13 to 16 CT image before the treatment, periapical X-ray image immediately after the treatment, at four months and atseven months (from left to right). iRaise is the right implant in the images.Figs. 17 to 22 The two remaining cases in the X-ray image before and a periapical image after the treatment. Figures 17 and 18show the right side of the first patient (pre-operative CT, post-operative periapical X-ray). Figures 19 to 22 show the right sideof the second patient (pre- and post-operative periapical X-rays). Figures 21 and 22 show the situation at the follow-up atfour months and at seven months.Discussion
The cases presented in this article demonstrate a
The author’s experience in the cases performed
new alternative to the open sinus lift, which may
show that the technique is easy to implement and
potentially provide the advantages of a simpler sur-
has a simple learning curve. The patients went
gical technique and reduced trauma and recovery
through the treatment easily and simply, with a
time for the patient. It is based on a hydraulic eleva-
good treatment experience, without significant dis-
tion procedure, combined within a dental implant
to allow a simultaneous elevation and implantation
These cases, however, represent preliminary expe-
rience with the surgical technique and are limitedto two patients and to four procedures. Once addi-tional patients have been treated, and with more
Contact address
extensive follow-up of the patients, the efficacy of
Eran Fermon, DMD
the method may be examined on a greater sample
of cases and the development of bone after the
Visit the web to find the list of references (www.teamwork-media.de). Follow the link “Literaturverzeichnis“ in the left sidebar.
24 de agosto de 2011 Lista Prohibida 2012 RESÚMEN de las PRINCIPALES MODIFICACIONES y NOTAS EXPLICATIVAS INTRODUCCIÓN Los miembros de la Comunidad Antidopaje deben saber que se ha prestado una meticulosa consideración a los pertinentes comentarios recibidos en respuesta a la distribución del borrador de la Lista 2012. Se hace salvedad que no todas las sugerenc
Nancy B. Davis, MDa, Ashesh B. Jani, MDb,aDepartment of Medicine, Section of Hematology/Oncology, The University of Chicago Medical Center,5841 South Maryland Avenue, MC2115, Chicago, IL 60637, USAbDepartment of Radiation and Cellular Oncology, The University of Chicago Medical Center,5841 South Maryland Avenue, MC 9006, Chicago, IL 60637, USAcThe Ben May Institute for Cancer Research, Th
 Clinical experience with a new implant in a minimally invasive procedure
Bilateral sinus floor elevation
Clinical experience with a new implant in a minimally invasive procedure
Bilateral sinus floor elevation 



 elevation and simultaneous implant insertion at
was raised by crestal incision, without release inci-
site 16 and another conventional implant insertion
sions. An osteotomy was prepared at site 26, and the
at site 17 were carried out, and sinus floor elevation
sinus floor was identified using a flat bur that pro-
and simultaneous implant insertion were per-
vides for tactile sensation of the hard cortical bone
formed at sites 26 (sinus lift implant) and 27 (con-
of the sinus floor, without any risk of rupture. After
ventional implant). The method provides for aug-
widening the bore, the sinus floor was weakened
mentation of a whole sinus using a single implant. If
using a specialized diamond bur. At this stage the
additional implants are required in the treated sinus,
implant was inserted into the bore. A tube connec-
conventional implants of any manufacture may be
tor was attached to the implant to enable the injec-
placed within the elevated space that already con-
tains bone graft material. In the cases described
The membrane was elevated by hydrostatic pres-
here, the conventional implants were iSure implants
sure by injecting 3 cm3 of normal saline solution
through the implant. The saline was removed from
Before treatment, the patient received prophy-
the sinus by withdrawing the syringe plunger and
lactic antibiotics (amoxicillin and clavulanic acid,
appeared to be mixed with a little blood (Fig. 4), a
875 mg) and performed a mouthwash (chlorhexidine
clinical indicator for the saline having come in con-
gluconate 0.12 %). A full-thickness mucoperiosteal flap
tact with the Schneiderian membrane, breachingthe small blood vessels between the membrane andthe sinus floor. Next, 3 cm3 of synthetic bone substi-tute were inserted (MBCP Gel, Biomatlante, France)(Fig. 5), selected because it is easily injected throughthe implant and is fairly radiopaque, allowing it tobe identified on post-operative X-rays.
The connector was removed and the implant fully
inserted into the bone. Beside the sinus lift implantat site 27, a conventional implant was placed usinga standard drilling protocol. This osteotomy wasdrilled directly into the sinus, inside the bone graftbeneath the elevated membrane. Figures 6 and 7
Figs. 6 and 7 CT scan before the treatment, periapical X-ray image after the treat-ment. iRaise is the left implant in the images.
show X-ray images before and after the treatment.
elevation and simultaneous implant insertion at
was raised by crestal incision, without release inci-
site 16 and another conventional implant insertion
sions. An osteotomy was prepared at site 26, and the
at site 17 were carried out, and sinus floor elevation
sinus floor was identified using a flat bur that pro-
and simultaneous implant insertion were per-
vides for tactile sensation of the hard cortical bone
formed at sites 26 (sinus lift implant) and 27 (con-
of the sinus floor, without any risk of rupture. After
ventional implant). The method provides for aug-
widening the bore, the sinus floor was weakened
mentation of a whole sinus using a single implant. If
using a specialized diamond bur. At this stage the
additional implants are required in the treated sinus,
implant was inserted into the bore. A tube connec-
conventional implants of any manufacture may be
tor was attached to the implant to enable the injec-
placed within the elevated space that already con-
tains bone graft material. In the cases described
The membrane was elevated by hydrostatic pres-
here, the conventional implants were iSure implants
sure by injecting 3 cm3 of normal saline solution
through the implant. The saline was removed from
Before treatment, the patient received prophy-
the sinus by withdrawing the syringe plunger and
lactic antibiotics (amoxicillin and clavulanic acid,
appeared to be mixed with a little blood (Fig. 4), a
875 mg) and performed a mouthwash (chlorhexidine
clinical indicator for the saline having come in con-
gluconate 0.12 %). A full-thickness mucoperiosteal flap
tact with the Schneiderian membrane, breachingthe small blood vessels between the membrane andthe sinus floor. Next, 3 cm3 of synthetic bone substi-tute were inserted (MBCP Gel, Biomatlante, France)(Fig. 5), selected because it is easily injected throughthe implant and is fairly radiopaque, allowing it tobe identified on post-operative X-rays.
The connector was removed and the implant fully
inserted into the bone. Beside the sinus lift implantat site 27, a conventional implant was placed usinga standard drilling protocol. This osteotomy wasdrilled directly into the sinus, inside the bone graftbeneath the elevated membrane. Figures 6 and 7
Figs. 6 and 7 CT scan before the treatment, periapical X-ray image after the treat-ment. iRaise is the left implant in the images.
show X-ray images before and after the treatment.



 Figs. 8 and 9Verification ofreaching thesinus floor byperiapical X-rayimage with adepth gauge.
Second patient
Figs. 8 and 9Verification ofreaching thesinus floor byperiapical X-rayimage with adepth gauge.
Second patient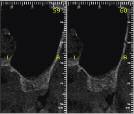




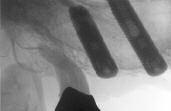



 Figs. 13 to 16 CT image before the treatment, periapical X-ray image immediately after the treatment, at four months and atseven months (from left to right). iRaise is the right implant in the images.
Figs. 17 to 22 The two remaining cases in the X-ray image before and a periapical image after the treatment. Figures 17 and 18show the right side of the first patient (pre-operative CT, post-operative periapical X-ray). Figures 19 to 22 show the right sideof the second patient (pre- and post-operative periapical X-rays). Figures 21 and 22 show the situation at the follow-up atfour months and at seven months.
Discussion
Figs. 13 to 16 CT image before the treatment, periapical X-ray image immediately after the treatment, at four months and atseven months (from left to right). iRaise is the right implant in the images.
Figs. 17 to 22 The two remaining cases in the X-ray image before and a periapical image after the treatment. Figures 17 and 18show the right side of the first patient (pre-operative CT, post-operative periapical X-ray). Figures 19 to 22 show the right sideof the second patient (pre- and post-operative periapical X-rays). Figures 21 and 22 show the situation at the follow-up atfour months and at seven months.
Discussion