Jama -- nevirapine and zidovudine at birth to reduce perinatal transmission of hiv in an african setting: a randomized controlled trial, july 14, 2004, taha et al. 292 (2): 202
Vol. 292 No. 2, July 14, 2004 Original Contribution This Article • Abstract Nevirapine and Zidovudine at Birth to Reduce Perinatal •PDF Transmission of HIV in an African Setting
• Send to a friend • Save in My Folder
A Randomized Controlled Trial
Taha E. Taha, MBBS, PhD; Newton I. Kumwenda, PhD; Donald R. Hoover, PhD;Susan A. Fiscus, PhD; George Kafulafula, MBBS, FCOG; Chiwawa Nkhoma, MSc;
Citing Articles
Samah Nour, MBBCh; Shu Chen, MSc; George Liomba, MBBS, FRCPath;
Paolo G. Miotti, MD; Robin L. Broadhead, MBBS, FRCP
ABSTRACT Related Content Context Antenatal counseling and human immunodeficiency virus (HIV) testing are
not universal in Africa; thus, women often present in labor with unknown HIV status • Similar articles in JAMAwithout receiving the HIVNET 012 nevirapine (NVP) regimen (a single oral dose of
Topic Collections
NVP to the mother at the start of labor and to the infant within 72 hours of birth). Objective To determine risk of mother-to-child transmission of HIV when either
standard use of NVP alone or in combination with zidovudine (ZDV) was administered • Alert me on articles by
to infants of women tested at delivery. Design, Setting, and Participants A randomized, open-label, phase 3 trial conducted between April 1, 2000, and March 15, 2003, at 6 clinics in Blantyre, Malawi, Africa. The trial included all infants born to 894 women who were HIV positive, received NVP intrapartum, and were previously antiretroviral treatment– naive. Infants were randomly assigned to NVP (n = 448) and NVP plus ZDV (n = 446). Infants were enrolled at birth, observed at 6 to 8 weeks, and followed up through 3 to 18 months. The HIV status of 90% of all infants was established at 6 to 8 weeks. Intervention Mothers received a 200-mg single oral dose of NVP intrapartum and infants received either 2-mg/kg oral dose of NVP or NVP (same dose) plus 4 mg/kg of ZDV twice per day for a week. Main Outcome Measures HIV infection of infant at birth and 6 to 8 weeks, and adverse events. Results The mother-to-child transmission of HIV at birth was 8.1% (36/445) in infants administered NVP only and 10.1% (45/444) in those administered NVP plus ZDV (P = .30). A life table estimate of transmission at 6 to 8 weeks was 14.1% (95% confidence interval [CI], 10.7%-17.4%) in infants who received NVP and 16.3% (95% CI, 12.7%-19.8%) in those who received NVP plus ZDV (P = .36). For infants not infected at birth and retested at 6 to 8 weeks, transmission was 6.5% (23/353) in those who received NVP only and 6.9% (25/363) in those who received NVP plus ZDV (P = .88). Almost all infants (99%-100%) were breastfed at 1 week and 6 to 8 weeks. Grades 3 and 4 adverse events were comparable; 4.9% (22/448) and 5.4% (24/446) in infants receiving NVP only and NVP plus ZDV, respectively (P = .76). Conclusions The frequency of mother-to-child HIV transmission at 6 to 8 weeks in our 2 study groups was comparable with that observed for other perinatal HIV intervention studies among breastfeeding women in Africa. The safety of the regimen containing neonatal ZDV was similar to that of a standard NVP regimen. INTRODUCTION Jump to Section
Mother-to-child transmission of human immunodeficiency virus (HIV) in sub-
Saharan Africa can be decreased with use of nevirapine (NVP) and zidovudine
(ZDV).1-3 Phase 1 and 3 studies have evaluated the pharmacokinetics, safety, and
efficacy of NVP among women and infants who received various ZDV regimens.4-6
Information on the efficacy of adding neonatal ZDV to a standard regimen of NVP
(the HIVNET 012 regimen of an intrapartum single 200-mg oral dose plus a singleinfant oral dose of 2 mg/kg1) is limited. This information is needed because mostwomen in sub-Saharan Africa do not receive antenatal antiretroviral treatment of ZDV or other regimensand present in labor with HIV status unknown. We hypothesized that in situations in which the mother istested for HIV at the time of presentation for delivery, giving 2 short drug regimens to the infant at birthwould be more effective in increasing viral suppression and thus reducing mother-to-child transmission ofHIV than a single regimen.7 Additionally, a dual regimen could limit development of antiviral resistance toNVP because this has been reported to occur rapidly and frequently in more than 40% of infants whoreceived a single NVP dose.8-9 With extensive evidence that substantial transmission occurs very lateduring gestation,10 it is difficult to assume that the impact of postexposure prophylaxis with ZDV,especially when combined with NVP (which has a long-acting effect),4, 11-12 will be limited only touninfected infants at birth.
We recently reported that postexposure prophylaxis with NVP plus ZDV only to the infant, without themother receiving intrapartum NVP, significantly reduced mother-to-child transmission of HIV byapproximately 36% in Malawi, Africa.13 In the current study, our goal was to assess mother-to-childtransmission when both mother and infant had received a standard NVP regimen compared with mother-to-child transmission when both mother and infant had received the same standard NVP regimen with theaddition of the infant receiving ZDV for a week. Jump to Section Study Design and Population
A randomized, open-label, phase 3 clinical trial was conducted at 6 clinics in the
city of Blantyre and its suburbs in Malawi, southeast Africa. Women included in this
study are termed early presenters because they arrived early to the labor ward and
thus time from admission to delivery (expected to deliver 4 or more hours after
arrival based on the initial clinical examination) was adequate to consent, HIVcounsel (pretest and posttest), and administer NVP (200-mg single dose orally) to those women foundinfected with HIV prior to delivery. A total of 288 (34.3%) of 840 women, with data on time of admissionand delivery, delivered in less than 4 hours from time of admission to the labor ward and distribution bystudy group was similar (145 [34.5%] of 420 in the NVP plus ZDV group and 143 [34.1%] of 420 in theNVP-only group). The 4-hour period was chosen based on practical and logistical reasons. Time of dosingwith NVP prior to delivery is important in that it is generally agreed that women should receiveintrapartum NVP at least 2 hours before delivery for the concentration to be high enough in infant cordblood to be protective.14 Women were eligible for enrollment if they provided written informed consent,were HIV positive, and the infant was not anemic (hemoglobin <10 g/dL), preterm, or had other disordersrequiring admission to the neonatal intensive care unit. Study staff interacting with the women werefemale study nurses. Randomization and Treatment
Infants were randomized to receive either NVP alone (2-mg/kg single oral dose) or NVP (same dose) plusZDV (4 mg/kg orally twice per day [vs 2 mg/kg 4 times per day, to simplify dosing and encouragecompliance] for 7 days). Each clinic was assigned a separate list of computer-generated random allocationnumbers (involving permuted blocks of 10 with a ratio of 1:1 allocation). For allocation concealment, the
randomization instructions were given to study nurses in sequentially numbered, opaque, sealedenvelopes, which were only opened when a woman had consented to enroll and the infant was determinedto be eligible for enrollment in the study. Used envelopes with the assignment instruction enclosed weresent to a central office and were regularly audited by the study coordinator.
Based on the random allocation instruction, the infant was administered the study treatments promptlyafter delivery, when having the ability to swallow fluids. The mothers and infants were typically dischargedwithin 6 to 48 hours after delivery. A study nurse directly administered NVP to the infant (according toweight) with the use of a fine calibrated tuberculin syringe, and also gave the first dose of ZDV to theinfant while still in the hospital, and any subsequent doses if the infant stayed for an extended period. Forinfants randomized to receive ZDV, the mother was given the remaining ZDV syrup in plastic bottlescontaining sufficient amounts for a total of 1 week and directed to give the remaining doses to the infantat home every day at morning and evening. To assess adherence, mothers were interviewed after 1 week,regarding a dosing information form (completed by a study nurse) involving the ascertainment of theexact number of doses administered to the infant. Empty bottles were collected but this source ofinformation was less complete. Enrollment, Study Procedures, and Follow-up
Routine medical care for mothers and their children and referral, when necessary, were provided in thestudy clinics. All mothers were given multivitamin tablets in the postnatal period. All infants receivedPneumocystis jiroveci pneumonia trimethoprim-sulfamethoxazole prophylaxis up to age of 6 months asrecommended in Malawi. Data on demographics, pregnancy, and intrapartum and delivery histories wereobtained at the time of birth. Follow-up visits were scheduled at 1 week and 6 to 8 weeks, and 3, 6, 9,12, 15, and 18 months. Unscheduled interim visits were allowed and documented. Data on adverse eventswere collected by using a clinical history form at every visit, including unscheduled visits. Laboratory Testing
For assessment of maternal HIV status, venous blood samples were tested by using a rapid HIV test(Determine HIV-1/2, Abbott Laboratories, Tokyo, Japan). The results were available in approximately 20 to30 minutes. All HIV-positive samples were confirmed by using an enzyme-linked immunosorbent assay(ELISA) HIV test (Wellcozyme, Murex Biotech Limited, Dartford Kent, England); these results wereavailable before discharge from the hospital or at the first postnatal follow-up visit. No Western blottesting was performed as World Health Organization guidelines15 recommend 2 tests (rapid and ELISA) insettings where HIV prevalence is high. After enrollment and before discharge from the hospital, maternalvenous blood specimens were obtained for syphilis testing and baseline measurement of HIV viral loadand a complete blood cell count. Those women who were reactive for syphilis were provided appropriatetreatment at no cost. Assessment of maternal viral load took place in the United States (University ofNorth Carolina, Chapel Hill) by using an HIV RNA assay (Roche Amplicor Monitor, Indianapolis, Ind). Complete blood cell count measurements were performed locally by using an analyzer (Coulter ACT DiffHematology Analyzer, Coulter Corp, Miami, Fla).
Infant heelprick blood specimens were collected on filter paper cards as described previously.16 Thesedried blood spots were used in HIV-1 RNA assays at birth and visits using nucleic acid sequence–basedamplification assay technology (NucliSens HIV-1 RNA QL assay, BioMerieux, Durham, NC). The testingoccurred in the United States (University of North Carolina, Chapel Hill) by laboratory staff unaware ofstudy treatment assignment. All 6- to 8-week samples were tested first and for those found positive, driedblood spot samples from birth were tested. If the dried blood spot specimen from birth was negative, the3-month visit specimen was tested to confirm the 6- to 8-week visit HIV RNA result. An infant wasidentified as HIV infected at 6 to 8 weeks if 2 separate specimens tested positive (samples from either 6-8weeks and birth or 6-8 weeks and 3 months). All HIV RNA positive tests were repeated on the samesample for confirmation (all were confirmed positive [either on the same sample or a separate sample];included were samples from infants lost to follow-up between 6 and 8 weeks and 3 months [13 did notreturn for the 3-month visit]). In some instances, testing was performed on later visit samples to furtherconfirm the infant's HIV status. Seven infants were tested at a later visit, specifically the 6-month visit. Ofthese, 2 were tested at 6 months to confirm an HIV RNA-positive test at the 6- to 8-week visit, and
tested positive at 6 months. The other 5 were HIV negative at birth, missed the 6- to 8-week and 3-month visits, but returned for the 6-month visit and were found to still be HIV RNA negative. Birth driedblood spots were also tested for infants who died or were lost to follow-up between birth and the 6- to 8-week visit; these infants were considered infected if they were HIV positive at birth. Counseling regardingthe HIV status of their infants was provided to mothers as soon as test results were available.
The safety of the intervention was monitored via venous blood samples obtained from all infants at birthand 6 weeks for complete blood cell count measurement using the analyzer. Alanine aminotransferase wasmeasured on specimens collected at birth and 6 weeks in infants at the start of the trial17 (ASCA AGIIChemistry System, Landmark Scientific Inc, Greensboro, NC). Of the NVP plus ZDV and NVP-only groupsof infants, 37 and 43, respectively, were tested for alanine aminotransferase at baseline, and 80 and 84,respectively, were tested at 6 weeks.17 The number tested at birth is smaller than at 6 weeks because ofdifficulties in obtaining unhemolyzed heelprick samples. Infants from another study13 involving NVP werealso tested.17 At time of testing, data from the HIVNET 012 study1 in Uganda indicated no major safetyconcerns with use of the single-dose NVP regimen but no such toxicity data were available from Malawi;therefore, a limited assessment was performed. More infants would have been tested had the data beensuggestive of toxicity. Assessment of Adverse Events
A clinical history form was used to record adverse events, including level of severity (mild, moderate,severe, or life-threatening) and relatedness to the intervention. Adverse event interpretation was based onthe National Institutes of Health Division of AIDS Toxicity Table.18 Regardless of relatedness, infant deathswere separately reported. Two independent pediatricians (members of the data and safety monitoringboard of this study) assessed on a regular basis all reported infant deaths to ascertain the most likelycauses. Laboratory monitoring of adverse events was based on complete blood cell count on all infantsand alanine aminotransferase measurements on a sample of these infants. Adverse event summaries werepresented to the data and safety monitoring board at the time of interim analyses. Statistical Analyses
Data were double entered for cross-verification, managed on site, and rechecked at the Johns HopkinsUniversity. An as-randomized analysis, subject to available data, was followed. Comparisons of treatmentgroups were performed for binary characteristics using proportions and exact tests; continuouscharacteristics were compared using means and t tests. The P values were all 2-sided. We calculated theproportion of infants infected at birth and the proportion of those infected at 6 to 8 weeks among thoseinfants not infected at birth and retested at 6 to 8 weeks. The primary outcome was overall HIV infectionat 6 to 8 weeks calculated by the life table approach19 as {1 – [(1 – proportion of infants infected atbirth) x (1 – proportion of those infants not infected at birth who became infected at 6 to 8 weeks)]}. TheGreenwood approach to estimation of variance of the survival function20-21 was used to calculateconfidence intervals for the survival estimate, and make statistical comparisons of survival estimates.
Logistic regression was used to adjust the comparisons of HIV infection at 6 to 8 weeks for maternal HIVviral load and other factors possibly related to HIV infection. Treatment groups were compared regardingsecondary censored binary outcomes such as mortality using Kaplan-Meier curves. Maternal viral load waslog10 transformed for a more symmetrical distribution having no outliers. Maternal viral load was alsoevaluated as a categorical variable by dividing it into approximate tertiles (<10 000 copies/mL, 10 000-99 999 copies/mL, and 100 000 copies/mL). In the final analysis, a cutoff of less than 100 000 copies/mLvs at least 100 000 copies/mL was used because transmission frequency was similar in lower viral loadcategories. A sample size of 890 infants (445 per group) was originally planned to have more than 80%power (even with 10% dropout) to detect a reduction of 6- to 8-week mother-to-child transmission (ininfants tested at 6 to 8 weeks) from 14% in the group without ZDV to 7% in the group with ZDV using anO'Brien-Fleming spending function with = .05 and 2 interim analyses. SAS statistical software version8.2 (SAS Institute Inc, Cary, NC) was used for all statistical analyses. P .05 was considered statisticallysignificant. Approvals and Monitoring
This study was approved by institutional review boards in Malawi (the University of Malawi College ofMedicine Research and Ethics Committee) and in the United States (the Johns Hopkins Bloomberg Schoolof Public Health Committee on Human Research). All women gave written informed consent for HIVtesting and enrollment. This study underwent monitoring by a 5-member data and safety monitoring boardwith expertise in clinical trials, clinical practice in Malawi, and statistics. Two independent scientists (aninternist and an internist/pharmacologist) from the University of Malawi with expertise in clinical practiceand clinical trials performed a 10-day monitoring of all study sites, including the clinics, laboratory, anddata entry site, as well as review of the study conduct and procedures in the first 6 months of the study. Jump to Section
Overall, from April 1, 2000, to March 15, 2003, 9469 early presenting women were
screened and 8575 women were excluded, of whom about 41% were HIV negative,
31% declined to speak with the counselor regarding counseling about HIV and the
study, and 28% did not fulfill inclusion criteria (Figure 1). Thus, 894 women were
enrolled and their infants randomized; 446 were randomized to NVP plus ZDV and
448 were randomized to NVP alone. Because the initial HIV test was a rapid test, 5women were excluded after the ELISA test was found negative (2 in the NVP plusZDV group and 3 in the NVP-only group). The excluded women were counseled again and followed up withtheir infants throughout the study. The baseline characteristics by study group were comparable (Table 1),with the exception of mode of delivery; more cesarean deliveries (mostly nonelective) were performed inwomen with infants in the NVP-only group (for the NVP plus ZDV group, 1 [0.24%] of 423 deliveries wereelective and for the NVP-only group, 1 [0.24%] of 421 deliveries were elective). There were no significantdifferences between the 2 groups in viral load and almost all infants were still breastfed by 1 week and 6to 8 weeks (Table 1). Figure. Study Flow of Participating Women and Infants
HIV indicates human immunodeficiency virus; NVP, nevirapine;ZDV, zidovudine; ELISA, enzyme-linked immunosorbent assay. *These women declined to speak with the counselor regardingcounseling about HIV and the study. View larger version (70K): View this table: Table 1. Comparison of Baseline Characteristics*
From maternal dosing with NVP to delivery, the median length of time was 4.2 hours (interquartile range[IQR], 2.3-8.5) in mothers of infants who received NVP and 3.9 hours (IQR, 2.5-8.0) in mothers of infantswho received NVP plus ZDV (Wilcoxon rank test, P = .54). There were no statistically significantdifferences between the 2 study groups when maternal NVP dosing time was dichotomized to less than 2hours and 2 hours or more (Table 1). Median times from birth to administration of NVP to the infant were9.5 hours (IQR, 4.9-16.0) and 9.3 hours (IQR, 4.7-15.4), respectively (Wilcoxon rank test, P = .47), forthe groups that received NVP only and received NVP plus ZDV. Based on the maternal histories taken,more than 90% of the infants randomized to ZDV received the complete ZDV regimen (14 doses).
Transmission was comparable at birth (ie, before the infants were differentially treated, with some
receiving NVP only and others receiving NVP plus ZDV); 36 (8.1%) of 445 infants who received NVP alonewere HIV positive at birth vs 45 (10.1%) of 444 infants who received NVP plus ZDV (P = .30; Table 2). Ininfants who were HIV negative at birth and retested at 6 to 8 weeks, the frequency of infection betweenbirth and 6 to 8 weeks was nearly identical for the 2 treatment groups; 6.5% in those infants whoreceived NVP alone and 6.9% in those who received NVP plus ZDV (P = .88). View this table: Table 2. Proportion of Infants With HIV Infection by Randomization Status*
Table 2 shows that the life table estimates of mother-to-child transmission at 6 to 8 weeks were 14.1%(95% confidence interval [CI], 10.7%-17.4%) in those infants who received a standard NVP regimen vs16.3% (95% CI, 12.7%-19.8%) for infants who received NVP plus ZDV, which corresponds to a risk ratioof 1.15 (95% CI, 0.84-1.60). Controlling for important risk factors known to influence mother-to-childtransmission (viral load at delivery, rupture of membranes 4 hours, and mode of delivery) did not changethe lack of association between treatment and overall HIV infection at 6 to 8 weeks (adjusted odds ratiofor NVP plus ZDV vs NVP alone, 1.19; 95% CI, 0.79-1.79; Table 3). Maternal NVP dosing time of less than2 hours was not significantly associated with mother-to-child transmission in the univariate analysis (oddsratio, 1.01; 95% CI, 0.65-1.86) and was thus not included in the adjusted model. View this table: Table 3. Factors Associated With HIV Infection in Infants at 6 to 8 Weeks
Maternal viral load, however, was strongly associated with transmission (adjusted odds ratio, 2.66; 95%CI, 1.95-3.63). There was also a clear trend of increase in mother-to-child transmission with increase inmaternal viral level in each of the treatment groups. In infants who received NVP only, the life tableestimate of 6 to 8 week transmission was 11.7% when maternal viral load was less than 100 000copies/mL and 21.5% when maternal viral load was 100 000 copies/mL or more (P = .03). In infants whoreceived NVP plus ZDV, transmission was 12.9% when maternal viral load was less than 100 000copies/mL and 25.9% when maternal viral load was 100 000 copies/mL or more (P = .01).
A limited number of infants who did not test positive at birth (n = 36 in the NVP plus ZDV group and n =56 in the NVP-only group) were not tested at 6 to 8 weeks because they died, missed the 6- to 8-weekvisit, or were lost to follow-up (Figure 1). In each study group, a similar number of infants (4 and 7,respectively) died by 6 to 8 weeks. Maternal viral load levels, an important determinant of mother-to-childtransmission, did not significantly differ by treatment group in those infants who did not return for the 6-to 8-week visit. For example, the median maternal viral load level for 35 infants who received NVP plusZDV and did not return for the 6- to 8-week visit was 33 838 copies/mL and for 53 infants who receivedNVP only and did not return for the 6- to 8-week visit, the median maternal viral load level was 24 460copies/mL (Wilcoxon rank test, P = .98); the differences in data from the data given in Figure 1 (36 and56, respectively) are due to missing data for viral load.
Safety analyses for infants enrolled in this study showed that numbers of grade 3 or 4 adverse events(severe or life-threatening) were similar between treatment groups (22 [4.9%] in 448 infants in the NVP-only group and 24 [5.4%] in 446 infants in the NVP plus ZDV group; P = .76). Less than 3% of adverseevents were determined to be probably or possibly related to the intervention in the entire study (6 casesof rash, 7 cases of various skin manifestations other than rash, 3 cases of sepsis, and 8 cases ofmiscellaneous conditions [fever, cough, diarrhea, and oral lesions]). Severe adverse events wereconsidered to be mainly due to infections; of the 46 grade 3 or 4 adverse events, 25 cases (54%) werecoded as pneumonia, diarrhea, or malnutrition possibly related to infections. Changes in laboratoryparameters of alanine aminotransferase and hemoglobin, packed cell volume, and other hematologicalindices were largely consistent with grade 1 (mild) toxicity.17 For example, based on the National
Institutes of Health Division of AIDS Toxicity Table 1 classifications of safety for children younger than 3months,18 of 670 infants with hemoglobin results available at 6 to 8 weeks in the study herein, 78% hadnormal results, and the hematological changes were mild in 12%, moderate in 7%, and severe(hemoglobin <7 g/dL) in 3%. Severe hematological changes were observed in 15 (4.39%) of 342 of theNVP plus ZDV group and 7 (2.13%) of 329 of the NVP-only group (Fisher exact test, P = .13).
Based on Kaplan-Meier analyses, survival probabilities were comparable for infants who only received NVPto those for infants receiving NVP plus ZDV at 12 months (89% if NVP was administered vs 90% if NVPplus ZDV was administered) and 18 months (85% vs 87%, respectively). Survival analyses were based on227 children in the NVP plus ZDV group and 240 in the NVP-only group for the 12-month Kaplan-Meiercurves, and 166 and 172 for the respective groups for 18-month analyses. There was no statisticallysignificant difference at 12 or 18 months (log rank P = .50 and P = .51, respectively). Attenuation infollow-up is due to deaths and other causes of attrition (loss to follow-up, lack of interest in the study,and moving out of study area). For 78 infants who died by 18 months, the main reported causes of deathwere pneumonia, malaria, gastroenteritis, malnutrition, septicemia, tuberculosis, and meningitis,accounting for more than 85% of reported causes of death. Jump to Section
A standard NVP regimen (single intrapartum dose to the mother and single oral
dose to the infant) achieved an overall (per life table estimate) 6- to 8-week
mother-to-child transmission of 14.1% (95% CI, 10.7%-17.4%). This is
comparable with that observed in the HIVNET 012 study22 in Uganda (11.8%; 95%
CI, 8.2%-15.5%), and the SAINT trial23 in South Africa, which included a maternal
postnatal NVP dose in addition to the standard mother/infant dosing (12.3% [95%CI, 9.7%-15.0%] overall rate at 8 weeks). Transmission at 6 to 8 weeks excludinginfections at birth in our study was similar for infants who received NVP only (6.5%) and those whoreceived NVP plus ZDV (6.9%). The small difference in overall transmission of 14.1% and 16.3% may bedue to residual difference in transmission at birth (8.1% in infants receiving only NVP and 10.1% in thosereceiving NVP plus ZDV). Transmission between birth and 6 to 8 weeks in infants who received a standardNVP regimen in our study (6.5%; 95% CI, 4.2%-9.6%) was also similar to that of the SAINT study(5.7%; 95% CI, 3.7%-7.8%).
Compared with the risk of mother-to-child transmission when a standard NVP regimen was used, additionof a short neonatal ZDV course to the NVP regimen did not lead to increased reduction in mother-to-childtransmission as we originally anticipated. However, safety results were comparable between the 2 studygroups that included and did not include ZDV in the prophylaxis regimen for infants. At the time this studywas designed, few antiretroviral options were available in sub-Saharan Africa and a dual prophylacticregimen was justifiable based on potential benefits and risks. Today more information is available. Forexample, the PETRA study24 provided safety and efficacy data on lamivudine in combination with ZDV, andthe SAINT study23 compared a combination of these drugs with NVP. The addition of lamivudine to shortintrapartum and neonatal regimens to increase efficacy and limit development of resistance to NVP shouldbe considered.25 Similar to our findings of a lack of an effect, an international study (PACTG 316 study) innonbreastfeeding women receiving antenatal antiretroviral treatment showed no additional benefit whenintrapartum and newborn NVP were administered.26 However, the risk of perinatal transmission wasextremely low in the PACTG 316 study, in which a substantial proportion of women received highly activecombinations of antiretroviral treatments antenatally, and 34% of women had elective cesarean delivery.
We do not know the exact biological or pharmacological explanations for why addition of a short neonatalZDV regimen to a standard NVP regimen did not lead to further reduction in mother-to-child transmission. The safety of NVP in the presence of ZDV has been shown in prior studies in which ZDV was used as thestandard of care in the United States, or when ZDV was started late during pregnancy and continuedpostpartum.5-6,26-27 No significant drug interactions have been reported when NVP is used as shortprophylaxis. The combination of NVP and ZDV previously reduced mother-to-child transmission when themother did not receive intrapartum NVP13 (ie, when the infant was not initially primed through an
intrapartum maternal dose) but did not achieve the same degree of protection in the study herein whenthe mother was dosed.
We speculate that in infants born to women who had intrapartum NVP, the effect of NVP is substantiallypowerful and cellular inhibition is maximal to the extent that addition of short course neonatal ZDV wouldhave no effect. On the other hand, in infants not exposed at all to NVP through the maternal route, bothZDV and NVP may initiate simultaneous inhibition of HIV; possibly ZDV starting earlier because of itsfaster absorption of approximately 1 hour after dosing28 and this inhibition being complemented by NVP,which has a long-acting effect.4, 11-12 We do not have data to support these arguments, but there havebeen studies that showed reduction in mother-to-child transmission with addition of NVP intrapartum6, 27in which the mothers were using ZDV during pregnancy for at least 4 weeks or more. Thus, possibly eitherhigher levels of ZDV in cord blood were achieved by the time NVP was administered intrapartum, orreductions in maternal viral load were already achieved. The additional reduction in mother-to-childtransmission when intrapartum NVP is administered to women who were taking antenatal ZDV for a longperiod may be due to a combination of several factors.
A limitation common to our studies (and other perinatal trials conducted more recently) is lack of a controlgroup in which both women and infants did not receive treatment. However, perhaps the historical rate of28% mother-to-child transmission that has been observed in Malawi29-30 might reflect what the mother-to-child transmission would have been in this population if no treatment had been administered. Potentialbias may arise from use of an open-label design. We opted not to conceal the treatments to simplify theregimens and because NVP was provided to all infants directly by a research nurse while in the hospital. Additionally, the ZDV regimen was administered for 1 week and with the exception of the first dose, alldoses were administered at home by the mother, and adherence reports might not have been accurate. However, the level of reported adherence was high (approximately 90%). Similar open-label designs werealso used in other HIV perinatal trials conducted in Africa, including the HIVNET 012 in Uganda1 and SAINTin South Africa.23 Also, in this study setting, in which resources are limited, diagnoses may be presumptiveand based on clinical judgment; thus, misclassifications are possible.
Our studies in Malawi suggest several possible options for prevention of HIV transmission in breastfedinfants and in the context of the resource constraints of sub-Saharan Africa. First, voluntary counselingand testing should be available early during pregnancy (or even before pregnancy), allowing HIV-infectedwomen and their infants to receive standard NVP prophylaxis (eg, a woman could self-administer NVPwhen labor contractions commence). Our current study and other studies in Africa1, 23 indicate that thisregimen appears to be safe and effective. Second, women who present at the labor ward with unknownHIV status should be tested and offered a standard NVP regimen (for both mother and infant), if time isadequate to counsel, test for HIV, and give intrapartum NVP (if indicated). Third, women arriving too lateto the labor ward to be counseled, tested for HIV, and treated intrapartum, should be tested postnatally,and if positive, their infants should be given postexposure prophylaxis. We published a study13 showingthat a regimen of NVP plus ZDV administered to the infant with the mother receiving no intrapartum NVPreduced mother-to-child transmission in Malawi. Other regimens to prevent mother-to-child transmissioncould be equally appropriate, based on prevailing circumstances and resources, or more effective, andshould also be given consideration,31 taking into account issues of possible resistance involvingantiretroviral drugs, such as NVP.8-9
In our study, the regimen that included ZDV in addition to a standard NVP regimen appeared to beequivalent to the standard NVP regimen. It could have more value if addition of ZDV limits the appearanceof resistance to NVP by reducing HIV replication while NVP concentration decreases. We do not have thisinformation yet, but testing for resistance is in progress. The costs of a standard dose of NVP for motherand infant previously,1 or as in the study herein, or postexposure prophylaxis of the infant alone with NVPplus ZDV13 is approximately equivalent (US $4-5); addition of a 7-day course of ZDV (for the infant) to astandard NVP regimen (for both mother and infant) approximately doubles the cost. These drugs,however, are becoming more and more accessible through governmental and nongovernmentalorganizations at no cost. Additional research should focus on evaluation of antiretroviral extendedregimens to prevent transmission of HIV via breastmilk and on treatment of the women. AUTHOR INFORMATION Jump to Section Corresponding Author: Taha E. Taha, MBBS, PhD, Department of Epidemiology,
Room E7138, Bloomberg School of Public Health, Johns Hopkins University, 615 N
Wolfe St, Baltimore, MD 21205 ([email protected]). Author Contributions: Dr Taha had full access to all of the data in the study and
takes responsibility for the integrity of the data and the accuracy of the dataanalysis. Study concept and design: Taha, Kumwenda, Hoover, Liomba, Broadhead. Acquisition of data: Taha, Kumwenda, Hoover, Fiscus, Kafulafula, Nkhoma, Broadhead. Analysis and interpretation of data: Taha, Kumwenda, Hoover, Fiscus, Nour, Chen, Miotti, Broadhead. Drafting of the manuscript: Taha, Kumwenda, Hoover, Fiscus, Nour, Chen, Broadhead. Critical revision of the manuscript for important intellectual content: Taha, Kumwenda, Hoover, Fiscus,Kafulafula, Nkhoma, Nour, Liomba, Miotti, Broadhead. Statistical analysis: Taha, Hoover, Chen. Obtained funding: Taha, Kumwenda. Administrative, technical, or material support: Taha, Kumwenda, Hoover, Fiscus, Kafulafula, Nkhoma,Nour, Liomba, Miotti, Broadhead. Study supervision: Taha, Kumwenda, Hoover, Kafulafula, Liomba, Broadhead. Funding/Support: This study was funded by AIDS FIRCA award 5R03TW01199 and supplement from the Fogarty International Center, National Institutes of Health, and by the Doris Duke Charitable Foundation. Role of the Sponsors: Dr Miotti is employed by the National Institutes of Health; however, the National Institutes of Health and the Doris Duke Charitable Foundation did not participate in the design and conduct of the study, in the collection, management, analysis, or interpretation of the data, or in the preparation, review, or approval of the manuscript. Acknowledgment: We thank the members of the data and safety monitoring board: Malcolm Molyneux, FRCP (chair), Sara White, PhD, Terrie Taylor, DO, Elizabeth Molyneux, FRCP, and Grace Malenga, MBBS. We also thank Richard Auty, FRCP, and Johnstone Kumwenda, MRCP, for their monitoring activities. We are indebted to the mothers and children who participated in this study. Author Affiliations: Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Md (Drs Taha, Kumwenda, and Nour, and Ms Chen); Department of Statistics and Institute for Health, Health Care Policy and Aging Research, Rutgers University, Piscataway, NJ (Dr Hoover); Department of Microbiology and Immunology, University of North Carolina, Chapel Hill (Dr Fiscus); College of Medicine, University of Malawi (Drs Kafulafula, Liomba, and Broadhead) and Johns Hopkins University-College of Medicine-Ministry of Health Research Project (Ms Nkhoma), Blantyre, Malawi; and Office of AIDS Research, National Institutes of Health, Bethesda, Md (Dr Miotti). REFERENCES Jump to Section
1. Guay LA, Musoke P, Fleming T, et al. Intrapartum and neonatal single-dose
nevirapine compared with zidovudine for prevention of mother-to-child transmission
of HIV-1 in Kampala, Uganda. Lancet. 1999;354:795-802. ISI | PUBMED
2. Dabis F, Msellati P, Meda N, et al. 6-month efficacy, tolerance, and acceptability
of a short regimen of oral zidovudine to reduce vertical transmission of HIV in
breastfed children in Cote d'Ivoire and Burkina Faso. Lancet. 1999;353:786-792.
FULL TEXT | ISI | PUBMED3. Wiktor SZ, Ekpini E, Karon JM, et al. Short-course oral zidovudine for prevention of mother-to-child
transmission of HIV-1 in Abidjan, Cote d'Ivoire. Lancet. 1999;353:781-785. FULL TEXT | ISI | PUBMED 4. Mirochnick M, Fenton T, Gagnier P, et al. Pharmacokinetics of nevirapine in human immunodeficiency virus type 1-infected pregnant women and their neonates. J Infect Dis. 1998;178:368-374. ISI | PUBMED 5. Mirochnick M, Siminski S, Fenton T, et al. Nevirapine pharmacokinetics in pregnant women and in infants after in utero exposure. Pediatr Infect Dis J. 2001;20:803-805. ISI | PUBMED 6. Lallemant M, Jourdain G, Le Coeur S, et al. Multicentre, Randomized Controlled Trial, Assessing the Safety and Efficacy of Nevirapine in Addition to Zidovudine for the Prevention of Perinatal HIV in Thailand: The Second IAS Conference on HIV Pathogenesis and Treatment, Paris, France, 13-16 July 2003. London, England: International Medical Press; 2003. 7. Centers for Disease Control and Prevention. Public Health Service Task Force recommendations for the use of antiretroviral drugs in pregnant women infected with HIV-1 for maternal health and for reducing perinatal HIV-1 transmission in the United States. MMWR Recomm Rep. 1998;47:1-30. PUBMED 8. Nolan M, Fowler MG, Mofenson LM. Antiretroviral prophylaxis of perinatal HIV-1 transmission and the potential impact of antiretroviral resistance. J Acquir Immune Defic Syndr. 2002;30:216-229. ISI | PUBMED 9. Martinson N, Morris L, Gray G, et al. HIV resistance and transmission following single-dose nevirapine in a PMTCT cohort. In: 11th Conference on Retroviruses and Opportunistic Infections; February 8-11, 2004; San Francisco, Calif. Abstract 38. 10. Kourtis AP, Bulterys M, Nesheim SR, Lee FK. Understanding the timing of HIV transmission from mother infant. JAMA. 2001;285:709-712. FREE FULL TEXT 11. Mirochnick M. Antiretroviral pharmacology in pregnant women and their newborns. Ann N Y Acad Sci. 2000;918:287-297. FREE FULL TEXT 12. Musoke P, Guay LA, Bagenda D, et al. A phase I study of the safety and pharmacokinetics of nevirapine in HIV-1 infected pregnant women and their neonates. AIDS. 1999;13:479-486. FULL TEXT | ISI | PUBMED 13. Taha TE, Kumwenda NI, Gibbons A, et al. Short postexposure prophylaxis in newborn babies to reduce mother-to-child transmission of HIV-1. Lancet. 2003;362:1171-1177. FULL TEXT | ISI | PUBMED 14. Mirochnick M, Dorenbaum A, Blanchard S, et al. Pre-dose infant nevirapine (NVP) concentration with the 2-dose intrapartum-infant NVP regimen. In: 3rd Conference on Global Strategies for the Prevention of HIV Transmission from Mothers to Infants; September 9-13, 2001; Kampala, Uganda. Abstract 101. 15. UNAIDS/WHO: Working Group on Global HIV/AIDS/STI Surveillance. Guidelines for using HIV testing technologies in surveillance. Available at: http://www.who.int/hiv/pub/surveillance/en/guidelinesforUsingHIVTestingTechs_E.pdf. Assessibility verified June 10, 2004. 16. Biggar RJ, Miley W, Miotti P, et al. Blood collection on filter paper: a practical approach to sample collection for studies of perinatal HIV transmission. J Acquir Immune Defic Syndr. 1997;14:368-373. PUBMED 17. Taha TE, Kumwenda N, Gibbons A, et al. Effect of HIV-1 antiretroviral prophylaxis on hepatic and hematological parameters of African infants. AIDS. 2002;16:851-858. FULL TEXT | ISI | PUBMED 18. Division of AIDS (DAIDS) Toxicity Table 1 for Grading Severity of Pediatric ( 3 Months of Age) Adverse Experiences. Available at: http://www.hptn.org/Web%20Documents/Regulatory_Resources/PediatricToxTablesLessthan3months.pdf. Accessibility verified June 4, 2004. 19. Chiang CL. The Life Table and Its Applications. Malabar, Fla: Robert E. Kreiger Publishing Co; 1984:156. 20. Greenwood M. The Errors of Sampling of the Survivorship Tables. London, England: Her Majesty's Stationery Office; 1926. Reports on Public Health and Statistical Subjects, No. 33. 21. Szklo M, Nieto FJ. Epidemiology: Beyond the Basics. Gaithersburg, Md: Aspen Publishers Inc; 2000:434. 22. Jackson JB, Musoke P, Fleming T, et al. Intrapartum and neonatal single-dose nevirapine compared with zidovudine for prevention of mother-to-child transmission of HIV-1 in Kampala, Uganda. Lancet. 2003;362:859-868. FULL TEXT | ISI | PUBMED 23. Moodley D, Moodley J, Coovadia H, et al. A multicenter randomized controlled trial of nevirapine versus a combination of zidovudine and lamivudine to reduce intrapartum and early postpartum mother- to-child transmission of human immunodeficiency virus type 1. J Infect Dis. 2003;187:725-735. FULL TEXT | ISI | PUBMED 24. The PETRA Study Team. Efficacy of three short-course regimens of zidovudine and lamivudine in preventing early and late transmission of HIV-1 from mother to child in Tanzania, South Africa, and Uganda (PETRA study). Lancet. 2002;359:1178-1186. FULL TEXT | ISI | PUBMED 25. Beckerman KP. Long-term findings of HIVNET 012. Lancet. 2003;362:842-843. FULL TEXT | ISI | PUBMED
26. Dorenbaum A, Cunningham CK, Gelber RD, et al. Two-dose intrapartum/newborn nevirapine and standard antiretroviral therapy to reduce perinatal HIV transmission. JAMA. 2002;288:189-198. FREE FULL TEXT 27. Gaillard P, Fowler MG, Dabis F, et al. Use of antiretroviral drugs to prevent HIV-1 transmission through breastfeeding. J Acquir Immune Defic Syndr. 2004;35:178-187. ISI | PUBMED 28. Boucher FD, Modlin JF, Weller S, et al. Phase I evaluation of zidovudine administered to infants exposed at birth to the human immunodeficiency virus. J Pediatr. 1993;122:137-144. ISI | PUBMED 29. Biggar RJ, Miotti PG, Taha TE, et al. Perinatal intervention trial in Africa: effect of a birth canal cleansing intervention to prevent HIV transmission. Lancet. 1996;347:1647-1650. FULL TEXT | ISI | PUBMED 30. Semba RD, Kumwenda NI, Hoover R, et al. Human immunodeficiency virus load in breastmilk, mastitis, and mother-to-child transmission of human immunodeficiency virus type 1. J Infect Dis. 1999;180:93-98. FULL TEXT | ISI | PUBMED 31. Public Health Service Task Force recommendations for use of antiretroviral drugs in pregnant HIV-1- infected women for maternal health and interventions to reduce perinatal HIV-1 transmission in the United States. Available at: http://www.aidsinfo.nih.gov. Accessibility verified June 4, 2004. RELATED ARTICLE Treatment of HIV/AIDS: Do the Dilemmas Only Increase? Merle A. Sande and Allan Ronald JAMA. 2004;292(2):266-268. EXTRACT | FULL TEXT THIS ARTICLE HAS BEEN CITED BY OTHER ARTICLES Suppression of Viremia and Evolution of Human Immunodeficiency Virus Type 1 Drug Resistance in a Macaque Model for Antiretroviral Therapy Ambrose et al. J. Virol. 2007;81:12145-12155. ABSTRACT | FULL TEXT Sensitivity of the ViroSeq HIV-1 Genotyping System for Detection of the K103N Resistance Mutation in HIV-1 Subtypes A, C, and D Church et al. J. Mol. Diagn. 2006;8:430-432. ABSTRACT | FULL TEXT Evidence behind the WHO Guidelines: Hospital Care for Children: What Antiretroviral Agents and Regimens are Effective in the Prevention of Mother-to-child Transmission of HIV? Nightingale and Dabis J Trop Pediatr 2006;52:235-238. FULL TEXT Persistence of nevirapine-resistant HIV-1 in women after single-dose nevirapine therapy for prevention of maternal-to-fetal HIV-1 transmission Palmer et al. Proc. Natl. Acad. Sci. USA 2006;103:7094-7099. ABSTRACT | FULL TEXT Affordable, Abbreviated Roche Monitor Assay for Quantification of Human Immunodeficiency Virus Type 1 RNA in Plasma Fiscus et al. J. Clin. Microbiol. 2005;43:4200-4202. ABSTRACT | FULL TEXT Prenatal Screening for HIV: A Review of the Evidence for the U.S. Preventive Services Task Force Chou et al. ANN INTERN MED 2005;143:38-54. ABSTRACT | FULL TEXT Gender Differences in Perinatal HIV Acquisition Among African Infants Taha et al. Pediatrics 2005;115:e167-e172. ABSTRACT | FULL TEXT
Reducing HIV Transmission from Mothers to Newborns JWatch Women's Health 2004;2004:5-5. FULL TEXT Interrupting Mother-to-Infant Transmission of HIV JWatch Infect. Diseases 2004;2004:1-1. FULL TEXT Treatment of HIV/AIDS: Do the Dilemmas Only Increase? Sande and Ronald JAMA 2004;292:266-268. FULL TEXT
HOME | CURRENT ISSUE | PAST ISSUES | TOPIC COLLECTIONS | CME | SUBMIT | SUBSCRIBE | HELP
CONDITIONS OF USE | PRIVACY POLICY | CONTACT US | SITE MAP
2004 American Medical Association. All Rights Reserved.
Level 10, 155 George St, Sydney NSW 2000 Australia Medication Competency This Medication competency paper has been designed to assess Registered Nurses and Endorsed Enrolled Nurses on their competency in relation to the calculation and the safe administration of medications. Every institution will have its own policies and guidelines in place for the safe administration of medications;
BIBLIOGRAPHIE DEMEURE Claude, Marketing , 4e édition, Paris, Sirey, 2003. ADAMI, Guide de la négociation des contrats d’artistes , Paris, Adami, 2005. DUDIGNAC Charlotte, MAUGER François, La Musique assiégée : d’une industrie en crise à APCE, Entreprendre dans le domaine musical , la musique équitable , Montreuil, L’Échappée, Paris, APCE, col . « Les fiches professionn

 Vol. 292 No. 2, July 14, 2004
Vol. 292 No. 2, July 14, 2004


 tested positive at 6 months. The other 5 were HIV negative at birth, missed the 6- to 8-week and 3-month visits, but returned for the 6-month visit and were found to still be HIV RNA negative. Birth driedblood spots were also tested for infants who died or were lost to follow-up between birth and the 6- to 8-week visit; these infants were considered infected if they were HIV positive at birth. Counseling regardingthe HIV status of their infants was provided to mothers as soon as test results were available.
tested positive at 6 months. The other 5 were HIV negative at birth, missed the 6- to 8-week and 3-month visits, but returned for the 6-month visit and were found to still be HIV RNA negative. Birth driedblood spots were also tested for infants who died or were lost to follow-up between birth and the 6- to 8-week visit; these infants were considered infected if they were HIV positive at birth. Counseling regardingthe HIV status of their infants was provided to mothers as soon as test results were available.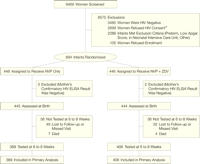 This study was approved by institutional review boards in Malawi (the University of Malawi College ofMedicine Research and Ethics Committee) and in the United States (the Johns Hopkins Bloomberg Schoolof Public Health Committee on Human Research). All women gave written informed consent for HIVtesting and enrollment. This study underwent monitoring by a 5-member data and safety monitoring boardwith expertise in clinical trials, clinical practice in Malawi, and statistics. Two independent scientists (aninternist and an internist/pharmacologist) from the University of Malawi with expertise in clinical practiceand clinical trials performed a 10-day monitoring of all study sites, including the clinics, laboratory, anddata entry site, as well as review of the study conduct and procedures in the first 6 months of the study.
This study was approved by institutional review boards in Malawi (the University of Malawi College ofMedicine Research and Ethics Committee) and in the United States (the Johns Hopkins Bloomberg Schoolof Public Health Committee on Human Research). All women gave written informed consent for HIVtesting and enrollment. This study underwent monitoring by a 5-member data and safety monitoring boardwith expertise in clinical trials, clinical practice in Malawi, and statistics. Two independent scientists (aninternist and an internist/pharmacologist) from the University of Malawi with expertise in clinical practiceand clinical trials performed a 10-day monitoring of all study sites, including the clinics, laboratory, anddata entry site, as well as review of the study conduct and procedures in the first 6 months of the study. receiving NVP only and others receiving NVP plus ZDV); 36 (8.1%) of 445 infants who received NVP alonewere HIV positive at birth vs 45 (10.1%) of 444 infants who received NVP plus ZDV (P = .30; Table 2). Ininfants who were HIV negative at birth and retested at 6 to 8 weeks, the frequency of infection betweenbirth and 6 to 8 weeks was nearly identical for the 2 treatment groups; 6.5% in those infants whoreceived NVP alone and 6.9% in those who received NVP plus ZDV (P = .88).
receiving NVP only and others receiving NVP plus ZDV); 36 (8.1%) of 445 infants who received NVP alonewere HIV positive at birth vs 45 (10.1%) of 444 infants who received NVP plus ZDV (P = .30; Table 2). Ininfants who were HIV negative at birth and retested at 6 to 8 weeks, the frequency of infection betweenbirth and 6 to 8 weeks was nearly identical for the 2 treatment groups; 6.5% in those infants whoreceived NVP alone and 6.9% in those who received NVP plus ZDV (P = .88). transmission of HIV-1 in Abidjan, Cote d'Ivoire. Lancet. 1999;353:781-785. FULL TEXT | ISI | PUBMED
transmission of HIV-1 in Abidjan, Cote d'Ivoire. Lancet. 1999;353:781-785. FULL TEXT | ISI | PUBMED