The Journal of Clinical Endocrinology & Metabolism 91(8):2960 –2966
Copyright 2006 by The Endocrine Society
Pegvisomant for the Treatment of gsp-Mediated Growth Hormone Excess in Patients with McCune-Albright Syndrome
Sunday O. Akintoye, Marilyn H. Kelly, Beth Brillante, Natasha Cherman, Sarah Turner,John A. Butman, Pamela G. Robey, and Michael T. Collins
Craniofacial and Skeletal Diseases Branch (S.O.A., M.H.K., B.B., N.C., P.G.R., M.T.C., S.T.) and Diagnostic RadiologyDepartment (J.A.B.), Clinical Center, National Institutes of Health, Department of Health and Human Services, Bethesda,Maryland 20892Context: GH excess affects approximately 20% of the patients with
in serum IGF binding protein-3 (IGFBP-3), improvement of fatigue
McCune-Albright syndrome (MAS). MAS is caused by sporadic,
and sweating, and reduction in markers of bone metabolism and bone
postzygotic, activating mutations in the GNAS gene, which codes for
the cAMP-regulating protein, G ␣ (gsp oncogene). These same mu-
tations are found in approximately one third of the sporadic cases of
Results: Combined mean changes in serum IGF-I at 6 and 12 wk were
Ϫ236.4 ng/ml (53%, P Ͻ 0.005) and Ϫ329.8 ng/ml (62%, P Ͻ 0.001),respectively. IGFBP-3 decreased by 0.8 mg/liter (24%, P Ͻ 0.01) and
Objective: We examined efficacy of the GH receptor antagonist,
2.9 mg/liter (37%, P Ͻ 0.005), respectively. There were no significant
pegvisomant, in controlling gsp oncogene-mediated GH excess and
changes in signs and symptoms of acromegaly or markers of bone
skeletal disease (fibrous dysplasia of bone) associated with MAS.
metabolism and bone pain, nor was there a significant change inpituitary size. Retrospective comparison of the degree of control
Setting and Patients: Five MAS patients with GH excess were
achieved with pegvisomant vs. other medications (long-acting oct-
treated with 20 mg/d sc injection of pegvisomant for 12 wk in a
reotide Ϯ dopamine agonist) in the same group showed that the two
randomized, double-blind, placebo-controlled crossover study at the
Conclusions: Pegvisomant effectively reduced IGF-I and IGFBP-3 Main Outcome Measures: The primary measure of efficacy was
levels in gsp-mediated GH excess but had no effect on fibrous
normalization of IGF-I. Secondary outcome measures were reduction
dysplasia. (J Clin Endocrinol Metab 91: 2960 –2966, 2006)
MCCUNE-ALBRIGHT SYNDROME (MAS) is classi- ever, the diagnosis of GH excess in MAS is sometimes dif-
cally defined clinically by the triad of polyostotic
ficult. In children with MAS, rapid linear growth as a sign of
fibrous dysplasia of bone (FD), cafe´-au-lait skin pigmenta-
GH excess is often ascribed to PP, which is seen in the
tion, and hyperfunctioning endocrinopathies, such as pre-
majority of patients with MAS. And whereas patients with
cocious puberty (PP), GH excess (acromegaly), hyperthy-
PP would be expected to have diminished final height, those
roidism, hypercortisolism, and renal phosphate wasting
with concomitant GH excess often attain (or exceed) the
associated with rickets/osteomalacia (1–3). The underlying
predicted midparental height. Therefore, normal stature in a
molecular etiology of MAS is a postzygotic mutation of the
person with MAS and PP can be a sign of GH excess (8). GNAS gene (R201H,C,S,G) that encodes for the ␣-subunit of
Additionally, the diagnosis is often delayed or missed be-
the stimulatory heterotrimeric G protein complex, G ␣
cause the characteristic coarsening of the face, frontal boss-
These result in a constitutive activation of the adenylyl cy-
ing, and prognathism evolve insidiously and may be ob-
clase enzyme signal transduction pathway and dysregulated
scured or attributed to the progression of the fibrous
production of cAMP (6). The constellation of phenotypic
dysplastic bone lesions in the skull, which themselves can
presentations seen in MAS is an example of mosaicism and
lead to some degree of dysmorphism in the absence of GH
results from the involvement of cells in the affected tissues
excess. It is important to diagnose and treat GH excess in
that harbor the gsp mutation and respond to the hormone-
MAS because GH excess is a risk factor for loss of vision and
sensitive adenylyl cyclase signal transduction pathway.
hearing (due to GH-fueled expansion of FD) as well as dra-
About 20% of MAS patients have GH excess (7, 8). How-
matic macrocephaly and dysmorphism (8, 9). First Published Online May 23, 2006
present in the adenomatous tissue of approximately one
Abbreviations: FD, Fibrous dysplasia of bone; IGFBP, IGF binding
third of the patients with sporadic acromegaly, suggesting
protein; LAR, long-acting sandostatin; MAS, McCune-Albright syn-
that these mutations may also be the molecular etiology in
drome; MRI, magnetic resonance imaging; OGTT, oral glucose tolerance
those sporadic cases of sporadic acromegaly. GH plays a
central role in skeletal development and maintenance, both
JCEM is published monthly by The Endocrine Society (http://www. endo-society.org), the foremost professional society serving the en-
through direct effects and those mediated by IGF-I (10). IGFs
docrine community.
circulate by binding to six different types of IGF binding
Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
TABLE 1. Demographics and clinical and molecular characterization of the study cohort
n/a, Not applicable; HT, hyperthyroidism; LT, Leydig cell tumor of testes; RPW, renal phosphate wasting; ST, Sertoli cell tumor of the testes;
a Substitution of the amino acid cysteine (Cys) or histidine (His) for arginine at position 201 determined from bone specimen. b See Ref. 14. c (30), 30 mg/month; DA, dopamine agonist; (), dose of cabergline per week.
proteins (IGFBPs), of which IGFBP-3 is the most abundant
MAS in normalizing serum IGF-I and, secondarily, its ability
(11, 12) and in some cases may be a sensitive marker for GH
to decrease serum IGFBP-3, signs and symptoms of GH ex-
cess, bone pain and markers of bone metabolism in the FD
Conventional treatments of GH excess include surgery,
medications, and radiotherapy. However, in patients withMAS, transphenoidal surgery is often not possible due to
Patients and Methods
massive thickening of the skull base with FD, and radiation
therapy is avoided because FD is prone to sarcomatous trans-
The study was a double-blinded, placebo-controlled, crossover study.
formation after radiation (13). Therefore, medical therapy is
Before enrollment, there was a 12-wk washout period during which all
often the only reasonable choice. Medical options include
medications for the treatment of GH excess were discontinued. Subjects
short- and long-acting analogs of somatostatin, dopamine
were randomized to either drug or placebo for 12 wk, after which there
receptor agonists, and more recently the GH receptor antag-
was a 6-wk washout period. Subjects were then crossed over to placeboor drug for the final 12 wk. The primary measure of pegvisomant efficacy
onist, pegvisomant. Somatostatin analogs and/or dopamine
was the age- and gender-specific normalization of serum IGF-I. Sec-
receptor agonists are not always effective in MAS (8), and it
ondary measures of efficacy were normalization of serum level of
is unclear whether controlling GH excess affects FD. In ad-
IGFBP-3, improvement in signs and symptoms of GH excess (sweating
dition, there has not been a report on the efficacy of a medical
and fatigue), decrease in serum and urine markers of bone metabolism,
treatment of GH excess in a population of patients whose
and a decrease in bone pain. Serum and urine samples were collectedat baseline and wk 6, 12, 18, 24, 30, and 36. Liver function tests, hemo-
disease is of a single molecular etiology. Therefore, we tested
gram, and electrocardiogram were performed to monitor for adverse
the efficacy of pegvisomant in a population of patients with
effects. Change in pituitary size was assessed as a measure of drug safety
IGF-I and head circumference. There was a sig-nificant association between head circumference(expressed as percent of the age- and gender-spe-cific upper limit of normal) and baseline serumIGF-I. This is a reflection of macrocephaly, a GHexcess-related morbidity in MAS.
J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
FIG. 2. Percent change of serum IGF-I during the course of the study.
The change in the serum IGF-I in comparison with the baseline (study
entry) value during the pegvisomant treatment (filled squares) andplacebo (open circles) phases are shown. During the pegvisomantphase, the serum IGF-I decreased an average of 63% from baseline.
Patient 4 experienced a 57% increase in serum IGF-I during the
course of the placebo phase of the study.
with magnetic resonance imaging (MRI) scanning at baseline and 1 yr.
Pegvisomant was kindly provided by Pfizer Inc. (New York, NY; Phar-
macia at the initiation of the study) as single-use, 20-mg strength ly-
ophilized powder that was reconstituted with 1 ml saline for injection.
Each vial of pegvisomant or placebo also contained 1.36 mg glycine, 36mg mannitol, 1.04 mg sodium phosphate, dibasic (anhydrous), and 0.36mg monobasic sodium phosphate. Both pegvisomant and placebo ap-
peared similar in color after reconstitution. When a patient was on
pegvisomant, the first dose was a loading dose of 40 mg followed by
daily sc administration of 20 mg. The study was approved by the In-
stitutional Review Board of the National Institute of Dental and Cranio-
facial Research, National Institutes of Health.
Five patients were studied. There were 10 patients (adults and chil-
dren) in the NIH cohort who were eligible for enrollment. Five declined
enrollment for personal reasons, which included unwillingness to dis-
continue medical treatment for the washout period. MAS was diagnosed
by a combination of clinical history; characteristic radiographic and
histological features of FD; endocrine testing; and, when necessary,
analysis of GNAS gene mutation. The age range was 13–39 yr, with a
mean of 28 yr (Table 1). GH excess was diagnosed by clinical signs and
symptoms of GH excess, elevated serum GH and IGF-I levels, but the
key criterion for the diagnosis was a serum GH that did not suppress
less than 1 ng/ml at 60 min on a standard oral glucose tolerance test
(OGTT). Patient 2 (Table 1) had a normal IGF-I at baseline but a GH that
did not suppress on OGTT and complications known to be associated
with GH excess; one optic nerve decompression, and six facial/sinus
operations. None of the patients had had pituitary surgery, due to the
fact that either a pituitary adenoma was not visualized or they were
considered inoperable due to the thickness of the skull base. None of the
patients had prior radiotherapy because radiotherapy is a risk factor for
transformation of FD to a malignancy (13) and is used only as a last
resort. All patients had significant skeletal disease burden of FD (14).
Four of the five patients had a history of other endocrine disorders, but
only three had a demonstrable pituitary adenoma by MRI (Table 1).
Serum IGF-I and IGFBP-3 were measured by RIA (Esoterix Inc.,
Austin TX). Serum lGF-I Z-scores were computed using reference ranges
specific for the IGF-I assay. Serum GH was measured using a commercial
immunochemiluminometric assay (Mayo Medical Laboratories, Roch-
ester, MN) that was modified to avoid cross-reactivity with pegviso-
mant. Antipegvisomant antibodies were measured by MDS Pharma
Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
FIG. 3. Sweating, fatigue, and pain scores. Patients keptweekly logs and recorded sweating and fatigue scores (A)and pain scores (B). The mean score Ϯ 1 SD for each patienton drug (filled bars) and placebo (open bars) are shown. Astandardized, validated tool for the assessment of sweatingand fatigue was used (see Refs. 15 and 16), and the BriefPain Inventory was used to assess pain. As a group, therewere no differences in sweating, fatigue, or pain, but twopatients had significantly more pain on drug than placebo.
Services (Montreal, Canada). Patients kept a weekly diary to record
circumference were compared with age and gender-matched controls
subjective impressions of fatigue and sweating using a visual analog
(18), Z-scores were calculated using assay-specific age and gender-
scale ranging from 0 (none) to 10 (worst) (15, 16). Physical examination
matched reference values (8), and Pearson’s linear regression was used
was performed at baseline and wk 12, 18, 30, and 36. Patients were
to evaluate correlations and degree of significance. Statistical analyses
followed up for at least 12 months after the end of the drug and placebo
were two sided, and P Ͻ 0.05 was regarded statistically significant. All
analyses were performed with JMP Windows NT 5.1 statistical package
Secondary skeletal effects of pegvisomant on FD were assessed by
measuring markers of bone metabolism and bone pain. Bone pain wasmeasured using a validated, subjective self-assessment tool developedby the American Pain Society, the Modified Brief Pain Inventory (17).
Bone metabolism markers (serum alkaline phosphatase, bone-specific
Pfizer Inc. (Pharmacia), manufacturer of pegvisomant, limited its role
alkaline phosphatase, osteocalcin, urine N-telopeptides of collagen, pyr-
to supply of drug, placebo, and funds for patient travel and certain
idinoline, and deoxypyridinoline cross-links) were measured by stan-
assays. Study design, coordination, patient care and testing, data anal-
dard commercially available assays (Mayo Medical Laboratories).
ysis, and manuscript preparation were the sole responsibilities of the
Pituitary volume was assessed by T1-weighted noncontrast and post-
contrast MRI of the brain performed at baseline and 12 months afterenrollment. From sagittal and coronal sequences, anterior-posterior,superior-inferior, and medial-lateral measurements were recorded at the
maximum dimension to estimate pituitary gland volume.
All patients had signs and symptoms of GH excess in-
cluding macrocephaly, the degree of which correlated withbaseline IGF-I levels (R ϭ 0.91, P Ͻ 0.05, Fig. 1). The mean
Pegvisomant and placebo primary efficacy data were accessed as
baseline IGF-I for the group was 491 ng/ml.
percentage change from baseline and compared using Fisher’s exact testor the 2 test for the comparison of proportions. Continuous measures
A daily dose of 20 mg pegvisomant for 12 wk successfully
were compared using the two sample t test. Measurements of head
reduced serum IGF-I in all patients at 6 wk [combined mean
TABLE 3. Serum GH and pegvisomant levels, and anti-pegvisomant antibodies
Mean change in GH compared with baseline (%)
P value (differences between placebo and pegvisomant)
J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
TABLE 4. Markers of bone metabolism
Normal range is in parentheses in first column. n/a, Not available. a No mean changes from baseline were statistically significant.
difference Ϫ263.4 ng/ml (Ϫ53%; P Ͻ 0.005)] and 12 wk
Successful medical treatment in this group is especially im-
[combined mean difference of Ϫ329.8ng/ml (Ϫ63%; P Ͻ
portant because these patients are usually not good candi-
0.001, Table 2)]. The differences in serum IGF-I between
dates for surgery due to massive thickening of the skull base
baseline or placebo and drug treatment for each patient,
with FD, and they are not good candidates for radiation
shown as percent changes from baseline, are depicted in Fig.
because FD can undergo sarcomatous transformation with
2. The decrease in IGFBP-3 at 6 wk was significant (combined
radiation treatment. The urgency for successful medical
mean difference 0.8 mg/liter (24%; P Ͻ 0.01), and 12 wk
treatment is intensified by the fact that GH excess in FD is an
[combined mean difference Ϫ2.0 mg/liter (37%; P Ͻ 0.001,
independent risk factor for the development of disfiguring
Table 2)], suggesting that serum IGF-I may be a better mea-
macrocephaly as well as vision and hearing loss, presumably
sure of pegvisomant efficacy. There was no significant dif-
due to GH-stimulated expansion of FD lesions.
ference in the degree of the acromegalic symptoms of fatigue
We show here that pegvisomant, a GH receptor antago-
and sweating between the drug and placebo phases (Fig. 3),
nist, is an effective treatment for GH excess in patients with
nor was there a correlation between the severity of these
MAS. It significantly lowered both serum IGF-I and IGFBP-3
symptoms and the degree of IGF-I elevation (data not
in all patients and normalized these values in all but one
shown). Average weekly bone pain score was significantly
patient. Whereas this was not a head-to-head trial comparing
higher in two patients during pegvisomant treatment, but as
the efficacy of pegvisomant with other therapies, the efficacy
a group there was no overall effect on pain (Fig. 3).
of pegvisomant was retrospectively compared with that of
There was no change in random serum GH at 6 or 12 wk,
LAR Ϯ cabergoline. As a group there was no difference in the
antibodies to pegvisomant were undetectable throughout
degree of control, but one patient (patient 4) whose IGF-I had
the study, and serum pegvisomant levels confirmed com-
not been normalized by a combination of LAR ϩ cabergoline
pliance with study drug use (Table 3).
was controlled on pegvisomant alone (Table 5). The single
The levels of the markers of bone metabolism were quite
patient whose IGF-I was not normalized by pegvisomant
high, but there was no significant effect of treatment on either
(patient 1) went on to be treated with a combination of both
markers of bone formation (alkaline phosphatase and osteo-
LAR and pegvisomant, and even with this combination, the
calcin) or resorption (N-telopeptide, pyridinoline, and de-
IGF-I did not normalize. This is different from what was seen
oxypyridinoline cross-links; Table 4).
One patient had an increase in pituitary volume over a
12-month period, but as a group, there was no change inpituitary volume (Fig. 4). All the patients completed thestudy with no adverse events.
The efficacy of pegvisomant on lowering serum IGF-I was
compared with the efficacy of the regimen patients were onbefore the study. Before the study, all patients were treatedwith long-acting sandostatin (LAR) Ϯ cabergoline. The meanpercent decreases in IGF-I by the pretrial regimen and thepegvisomant were 52 and 63%, respectively (Table 5). Onepatient who had not been controlled by LAR ϩ cabergolinewas controlled by pegvisomant alone. Discussion
The medical treatment of a group of patients with GH
excess in the context of MAS offers the unique opportunity
FIG. 4. Pituitary volume. The pituitary volume was assessed by MRI
to study the effects of a drug in a group of acromegalic
at baseline and 12 months later. As a group there was no change in
patients whose disease is of a single molecular etiology, gsp.
Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
TABLE 5. Comparison of response to pretrial medication (Rx) and pegvisomant a LAR, Long-acting somatostatin agonist sandostatin LAR. b CAB, Dopamine agonist cabergoline. c P ϭ 0.13 for difference between pretrial medication (Rx) and pegvisomant.
in an earlier study that reported additive effects of pegvi-
Given the potential for tumor shrinkage by LAR and the
somant in combination with long-acting somatostatin ana-
established long-term safety of long-acting somatostatin an-
logs (19). It should be noted that this patient’s weight was 127
alogs, our recommendation for the initial treatment of GH
kg, and his baseline GH and IGF-I were very high, 75.6 and
excess in MAS is a trial of LAR. If this response is inadequate,
734 ng/ml, respectively. Given his large body mass and very
high-dose dopamine agonist or pegvisomant may be added.
high baseline GH and IGF-I values, it is possible that the fixed
If medical therapy is inadequate, and access to the pituitary
dose (by protocol) of pegvisomant may not have been suf-
is not prohibited by bone overgrowth, surgery may be an
ficient to call this a pegvisomant failure. Interestingly, in this
option. However, even in cases wherein it appears that a
group of patients, there was not a significant increase in the
single, discreet adenoma is the cause of excess GH, the gland
serum GH while on pegvisomant (Table 3), as had been
is often diffusely involved with areas of somatotroph hy-
reported in other studies (20, 21). The reason for this differ-
perplasia, and the only option for surgical cure is total hy-
ence is not known but could reflect that feedback inhibition
phophysectomy. The remaining option is radiation, which
is lost at baseline in gsp-mediated acromegaly and that when
should also be approached with caution because FD, which
IGF-I is lowered by pegvisomant, there is no further loss of
always encases the pituitary in MAS, is prone to sarcomatous
feedback inhibition and thus no increase in serum GH.
transformation after treatment doses of radiation (13). This
Whereas pegvisomant seems to be marginally better than the
risk may be minimized with technologies using focused
pretrial medical regimen, there was no significant difference
in response to therapy in patients with gsp-mediated GH
In summary, pegvisomant effectively controlled GH ex-
cess in patients with MAS and was at least as effective as LAR
Although pegvisomant lowered serum IGF-I and IGFBP-3,
it was disappointing that the drug had no effect on the GHexcess-related symptoms of fatigue and sweating. It is pos-
Acknowledgments
sible that this lack of effect was due to either the relatively
The authors express their gratitude to Ms. Susan Booher and Judith
short duration of treatment or the fact that the dose of pegvi-
Starling for their professional support. We thank the National Institutes
somant was not titrated to relief of symptoms. It was reas-
of Health Interinstitute Endocrine Training Program Fellows and the
suring that attenuation of the inhibitory feedback effect of
nurses of the National Institutes of Health Clinical Center for the su-
high IGF-I caused no change in pituitary volume as a group,
at least during the period under study. It is possible thatprogression in tumor size that was observed in one patient
Received December 8, 2005. Accepted May 16, 2006. Address all correspondence and requests for reprints to: Sunday O.
may be the result of disease progression. This point may be
Akintoye, B.D.S., D.D.S., M.S., University of Pennsylvania, School of
a reflection of the relatively short study length; therefore, as
Dental Medicine, Department of Oral Medicine, The Robert Schattner
in other medical treatments of GH excess, tumor size should
Center Room, 209, 240 South 40th Street, Philadelphia, Pennsylvania
be monitored in patients on chronic pegvisomant treatment.
19104. E-mail: [email protected].
This work was supported by the intramural program of the National
One of the expectations of this study was that the blockade
Institute of Dental and Craniofacial Research, National Institutes of
of GH receptors or the secondary lowering of serum IGF-I
Health (Bethesda, MD), and Pfizer Inc. (Pharmacia) (New York, NY).
would improve FD symptoms as assessed by a decrease in
Current address for S.A.O.: Department of Oral Medicine, University
bone pain and/or a decrease in markers of bone metabolism.
of Pennsylvania, School of Dental Medicine, Philadelphia, Pennsylvania.
Whereas there was a trend toward lower levels of markersof bone metabolism, this was not statistically significant,
References
perhaps attributable to the small number of patients studied
1. McCune DJ 1936 Osteitis fibrosa cystica: the case of a nine-year-old girl who
(Table 4). This is somewhat surprising, given the fact that
also exhibits precocious puberty, multiple pigmentation of the skin and hy-perthyroidism. Am J Dis Child 52:743–744
previous studies have shown that treatment of acromegalic
2. Albright F, Butler AM, Hampton AO, Smith P 1937 Syndrome characterized
patients, in whom markers of bone turnover were high at
by osteitis fibrosa disseminata, areas, of pigmentation, and endocrine dys-
baseline, with pegvisomant resulted in reductions of markers
function, with precocious puberty in females: report of 5 cases. N Engl J Med216:727–746
of bone turnover (22–24). In addition, there was no improve-
3. Collins MT 2004 McCune-Albright syndrome. Orphanet Online Database of
ment in bone pain, and in fact two patients experienced a
Rare Diseases (http://www.orpha.net), INSERM SCII; Paris
significant increase in bone pain. It is not clear whether this
4. Weinstein LS, Shenker A, Gejman PV, Merino MJ, Friedman E, Spiegel AM
1991 Activating mutations of the stimulatory G protein in the McCune-Al-
was related to drug effect or disease progression.
bright syndrome. N Engl J Med 325:1688 –1695
J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
5. Schwindinger WF, Francomano CA, Levine MA 1992 Identification of a Huber SL 1999 The rapid assessment of fatigue severity in cancer patients: use
mutation in the gene encoding the alpha subunit of the stimulatory G protein
of the Brief Fatigue Inventory. Cancer 85:1186 –1196
of adenylyl cyclase in McCune-Albright syndrome. Proc Natl Acad Sci USA
17. Premawardhana LD, Vora JP, Mills R, Scanlon MF 1992 Acromegaly and its
treatment in the McCune-Albright syndrome. Clin Endocrinol (Oxf) 36:605–
6. Spiegel AM 1997 The molecular basis of disorders caused by defects in G
18. Gorlin RJ, Cohen MM, Levin LS 1990 Syndromes of the head and neck. 3rd
7. Ringel MD, Schwindinger WF, Levine MA 1996 Clinical implications of
genetic defects in G proteins. The molecular basis of McCune-Albright syn-
19. Jorgensen JO, Feldt-Rasmussen U, Frystyk J, Chen JW, Kristensen LO, Ha-
drome and Albright hereditary osteodystrophy. Medicine (Baltimore) 75:171–
gen C, Orskov H 2005 Cotreatment of acromegaly with a somatostatin analog
and a growth hormone receptor antagonist. J Clin Endocrinol Metab 90:5627–
8. Akintoye SO, Chebli C, Booher S, Feuillan P, Kushner H, Leroith D, Cher- man N, Bianco P, Wientroub S, Robey PG, Collins MT 2002 Characterization
20. Trainer PJ, Drake WM, Katznelson L, Freda PU, Herman-Bonert V, van der
of gsp-mediated growth hormone excess in the context of McCune-Albright
Lely AJ, Dimaraki EV, Stewart PM, Friend KE, Vance ML, Besser GM,
syndrome. J Clin Endocrinol Metab 87:5104 –5112
Scarlett JA, Thorner MO, Parkinson C, Klibanski A, Powell JS, Barkan AL,
9. Uwaifo GI, Robey PG, Akintoye SO, Collins MT 2001 Clinical picture: fuel Sheppard MC, Malsonado M, Rose DR, Clemmons DR, Johannsson G, Bengtsson BA, Stavrou S, Kleinberg DL, Cook DM, Phillips LS, Bidling-
10. Ueland T 2005 GH/IGF-I and bone resorption in vivo and in vitro. Eur J maier M, Strasburger CJ, Hackett S, Zib K, Bennett WF, Davis RJ 2000
Treatment of acromegaly with the growth hormone-receptor antagonist pegvi-
11. Spagnoli A, Rosenfeld RG 1996 The mechanisms by which growth hormone
brings about growth. The relative contributions of growth hormone and in-
sulin-like growth factors. Endocrinol Metab Clin North Am 25:615– 631
21. Herman-Bonert VS, Zib K, Scarlett JA, Melmed S 2000 Growth hormone
12. Grinspoon S, Clemmons D, Swearingen B, Klibanski A 1995 Serum insulin-
receptor antagonist therapy in acromegalic patients resistant to somatostatin
like growth factor-binding protein-3 levels in the diagnosis of acromegaly.
analogs. J Clin Endocrinol Metab 85:2958 –2961
22. Wilson ME 2000 Insulin-like growth factor I (IGF-I) replacement during
13. Ruggieri P, Sim FH, Bond JR, Unni KK 1994 Malignancies in fibrous dys-
growth hormone receptor antagonism normalizes serum IGF-binding pro-
tein-3 and markers of bone formation in ovariectomized rhesus monkeys. J Clin
14. Collins MT, Kushner H, Reynolds JC, Chebli C, Kelly MH, Gupta A, Bril- lante B, Leet AI, Riminucci M, Robey PG, Bianco P, Wientroub S, Chen CC
23. Fairfield WP, Sesmilo G, Katznelson L, Pulaski K, Freda PU, Stavrou S,
2005 An instrument to measure skeletal burden and predict functional out-
Kleinberg D, Klibanski A 2002 Effects of a growth hormone receptor antag-
come in fibrous dysplasia of bone. J Bone Miner Res 20:219 –226
onist on bone markers in acromegaly. Clin Endocrinol (Oxf) 57:385–390
15. Schnider P, Binder M, Kittler H, Birner P, Starkel D, Wolff K, Auff E 1999
24. Parkinson C, Kassem M, Heickendorff L, Flyvbjerg A, Trainer PJ 2003
A randomized, double-blind, placebo-controlled trial of botulinum A toxin for
Pegvisomant-induced serum insulin-like growth factor-I normalization in pa-
severe axillary hyperhidrosis. Br J Dermatol 140:677– 680
tients with acromegaly returns elevated markers of bone turnover to normal.
16. Mendoza TR, Wang XS, Cleeland CS, Morrissey M, Johnson BA, Wendt JK, JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the endocrine community.
CASA CIVIL DA PRESIDÊNCIA DA REPÚBLICA SECRETARIA EXECUTIVA/ARQUIVO NACIONAL COORDENAÇÃO REGIONAL NO DISTRITO FEDERAL Eu, _______________________________________________________________________________________, portador(a) da Carteira de Identidade nº_____________________________________, expedida pela _________, e do CPF nº__________________, filho(a) de_____________________
 Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
TABLE 1. Demographics and clinical and molecular characterization of the study cohort
Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
TABLE 1. Demographics and clinical and molecular characterization of the study cohort J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
FIG. 2. Percent change of serum IGF-I during the course of the study.
J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
FIG. 2. Percent change of serum IGF-I during the course of the study.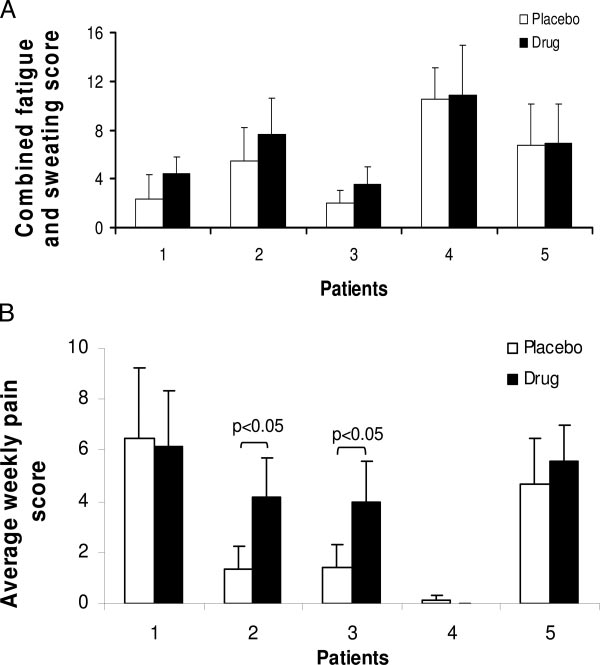 Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
FIG. 3. Sweating, fatigue, and pain scores. Patients keptweekly logs and recorded sweating and fatigue scores (A)and pain scores (B). The mean score Ϯ 1 SD for each patienton drug (filled bars) and placebo (open bars) are shown. Astandardized, validated tool for the assessment of sweatingand fatigue was used (see Refs. 15 and 16), and the BriefPain Inventory was used to assess pain. As a group, therewere no differences in sweating, fatigue, or pain, but twopatients had significantly more pain on drug than placebo.
Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
FIG. 3. Sweating, fatigue, and pain scores. Patients keptweekly logs and recorded sweating and fatigue scores (A)and pain scores (B). The mean score Ϯ 1 SD for each patienton drug (filled bars) and placebo (open bars) are shown. Astandardized, validated tool for the assessment of sweatingand fatigue was used (see Refs. 15 and 16), and the BriefPain Inventory was used to assess pain. As a group, therewere no differences in sweating, fatigue, or pain, but twopatients had significantly more pain on drug than placebo. J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
TABLE 4. Markers of bone metabolism
J Clin Endocrinol Metab, August 2006, 91(8):2960 –2966
Akintoye et al. • Pegvisomant for gsp-Mediated GH Excess
TABLE 4. Markers of bone metabolism