Brief reports 309 Allergic contact dermatitis to topical minoxidil solution: Etiology and treatment
Edward S. Friedman, BS, Paul M. Friedman, MD, David E. Cohen, MD MPH, and
Ken Washenik, MD, PhD New York, New York
After more than a decade of use, topical minoxidil solution has proven to be a safe and effective treatmentfor androgenetic alopecia. However, some patients present with complaints of pruritus and scaling of thescalp. The most common causes of these symptoms include irritant contact dermatitis, allergic contactdermatitis, or an exacerbation of seborrheic dermatitis. Patients suffering from allergic contact dermatitismay benefit from patch testing to determine the causative allergen. Among the patients we patch tested,propylene glycol was found to be the contactant in a majority of cases, not the minoxidil itself. Many ofthese patients may be candidates for treatment with alternative formulations using other solvents, such asbutylene glycol, polysorbate, or glycerol. Although predictive, patch testing results do not ensure that thecompounded preparations will be tolerated. Unfortunately, patients found to be allergic to minoxidil are nolonger candidates for topical treatment of their alopecia with any preparations of minoxidil. (J Am AcadDermatol 2002;46:309-12.)
Topical minoxidil solution is a hypertrichotic mulation and in 1.9% of the patients using the 2%
agent used to treat androgenetic alopecia
formulation.4 These included pruritus, erythema,
(AGA). AGA results from miniaturization of
hair follicles in androgen-sensitive areas of the scalp
in genetically predisposed persons.1 Arresting the
include irritant contact dermatitis, allergic contact
process of miniaturization remains the goal of med-
dermatitis, or an exacerbation of seborrheic der-
ical treatment. Currently topical minoxidil solution
matitis. Differentiation of these conditions is neces-
(minoxidil, alcohol, propylene glycol, and purified
sary for appropriate intervention because successful
water) and oral finasteride are the only therapies for
treatment of the local adverse reaction is necessary
this condition approved by the Food and Drug
for the patient to continue using topical minoxidil in
Administration.2 Topical minoxidil solution is
the treatment of their alopecia. This report focuses
approved for this indication in 2% and 5% formula-
on a series of patients whose presentation was most
tions. Although minoxidil functions as a vasodilator
consistent with an allergic contact dermatitis. The
when used systemically for hypertension, its mech-
goal in these patients was to utilize patch testing to
anism of action in hair loss involves a direct stimu-
elucidate the specific causative allergen involved.
latory effect on dermal papillae or follicular hair
Identifying the specific contactant may allow contin-
uation of the patient’s therapy with an alternative
Topical minoxidil solution has a favorable safety
profile and is currently available over the counter. The adverse effects of topical minoxidil solution are
SELECTED CASE REPORTS
predominantly dermatologic and limited to the
Case 1. A 67-year-old woman with a history of
scalp. The phase III clinical trial listed application site
AGA treated with topical minoxidil solution present-
reactions in 5.7% of the patients using the 5% for-
ed with mild erythema and scaling of the scalp. Shewas patch tested to a series of allergens and demon-strated a positive reaction to propylene glycol. Noreaction to butylene glycol or minoxidil was noted.
From The Ronald O. Perelman Department of Dermatology, New
These results indicated that a propylene glycol–free
preparation might have utility. The compounded for-
mulation substituted butylene glycol for propylene
Reprints not available from authors.
glycol. At 10 months, the patient was satisfied with
Copyright 2002 by the American Academy of Dermatology, Inc.
the efficacy and tolerability of the compounded for-
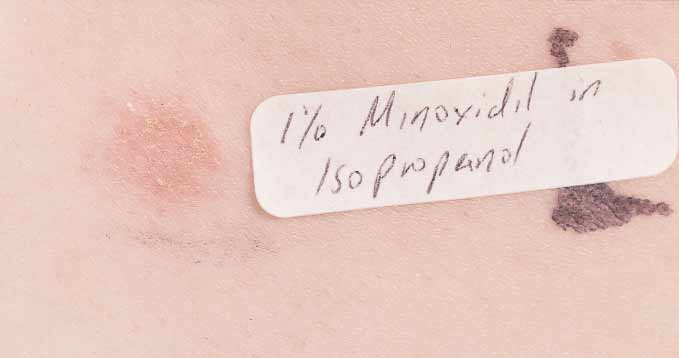
16/54/119104 310 Brief reports Fig 1. Positive allergic contact reaction to 1% minoxidil in isopropanol demonstrated by patch testing. Case 2. A 52-year-old woman using topical
Patients with a diagnosis of either irritant contact
minoxidil solution to treat her hair loss presented
dermatitis or seborrheic dermatitis can be effective-
with a complaint of increased scaling and scalp pru-
ly treated with anti-inflammatory agents including tar
ritus. Patch testing revealed an allergy to propylene
shampoo or topical corticosteroids while continuing
glycol, but no reaction to butylene glycol or minoxi-
their use of topical minoxidil solution. The subset of
dil. Despite these patch testing results, she was
patients diagnosed as having suspected allergic con-
unable to tolerate the compounded formulation
tact dermatitis should be patch tested to determine
because of continued scaling and pruritus at the
whether the allergen is the active ingredient minoxi-
dil or the solvent propylene glycol. Case 3. A 63-year-old man treating his AGA with
Eight additional patients were patch tested in the
5% topical minoxidil solution complained of
same manner as the patients described in the case
increased pruritus and scaling of the scalp. His pres-
reports. In total, there were 7 women and 4 men in
entation was consistent with allergic contact der-
the group, with an average age of 46.7 years. Nine of
matitis, and patch testing was performed. The
11 patients (81.8%) showed a positive allergic reac-
results demonstrated a positive reaction to minoxidil
tion to propylene glycol by patch testing. Two of the
(Fig 1). As a result, he was no longer a candidate for
9 were negative (ie, not sensitive) at a lower concen-
using topical minoxidil solution to treat his hair loss.
tration and positive (ie, sensitive) at a higher con-centration of propylene glycol. One of 11 patients
DISCUSSION
(9.1%) was reactive to butylene glycol, and 4 of 11
Topical minoxidil solution is an effective treat-
patients (36.4%) reacted to the active ingredient
ment for regrowth of hair in some patients and sta-
bilizes hair loss and miniaturization in a majority of
Among the patients we patch tested, propylene
them.5 Long-term application is required for contin-
glycol was found to be the agent most frequently
ued benefit. As with long-term exposure to any
responsible for allergic contact dermatitis to minoxi-
medicament, over time some patients may develop
dil solution. Two patients in our series demonstrated
contact dermatitis to a specific ingredient in the
a threshold sensitivity because they only reacted to a
preparation. Although the safety profile of topical
higher concentration of propylene glycol. This con-
minoxidil solution is favorable, the most common
cept is evident in previous patch test studies,6-9 in
complaint among users is scalp pruritus and scaling.
which increasing concentrations of propylene glycol
In addition to irritant and allergic contact dermatitis,
are less well tolerated. Paradigms for elicitation
these symptoms may be due to an exacerbation of
thresholds for allergic and irritant contact dermatitis
seborrheic dermatitis. While clinically similar, these
have been described.8-11 Thus there is utility in using
entities must be differentiated for optimal treatment
the lowest possible solvent concentration in prepa-
outcome and, more importantly, to allow the patient
rations for patients with a history of allergic or irri-
to continue treating his or her hair loss. Brief reports 311 Table I. Patch test results for 11 patients suspected of having an allergic contact reaction to topical minoxidil solution Patient No. Age (y)/Sex Propylene glycol Butylene glycol Minoxidil
*Started on compounded preparation. †Positive at 50%, negative at 20% concentration. ‡Positive at 50%, negative at 10% concentration.
Data from the phase III clinical trial for 2% and 5%
lene glycol, glycerin and polysorbate are possible
topical minoxidil solution support the concept of
alternative solvents.20,21 Given the concept of
threshold sensitivity. The 5% minoxidil formulation,
threshold elicitation demonstrated in our series, as
which contains more propylene glycol (50%) than
well as in previous studies, there is utility in using
the 2% minoxidil formulation (30%), was associated
the lowest solvent concentration required to solubi-
with a higher number of cases of itching, erythema,
and dryness. This difference is not due to the minox-
No clinical studies have been performed compar-
idil concentration because the patients using the
ing the efficacy of topical minoxidil prepared with
vehicle with 50% propylene glycol reported a similar
alternative solvents. However, these preparations
incidence of adverse events to the patients using the
provide a method for delivering minoxidil to the
scalps of propylene glycol–sensitive patients.
Previous reports have suggested that the active
Because topical minoxidil solution is the only Food
ingredient, minoxidil, was the more common aller-
and Drug Administration–approved topical treatment
gen.12-18 However, it should be noted that the series
for AGA, the treatment options for hair loss in these
of allergens utilized in these studies were not con-
patients are very limited. Patients suspected of suffer-
sistent and the patient numbers were small. Our
ing from allergic contact dermatitis should be advised
patch test study was specifically designed to deter-
to undergo patch testing to determine the causative
mine whether each individual patient was allergic to
allergen. If the patients are found to be sensitive to
propylene glycol, then they should be given the
Patients found to be allergic to propylene glycol
option of formulations compounded with alternative
were candidates for compounded preparations of
solvents. Unfortunately, patients found to be allergic
topical minoxidil formulated without propylene gly-
to minoxidil are no longer candidates for the topical
col. For these patients, we chose butylene glycol
treatment of their alopecia with minoxidil; our data
when possible as a substitute. Chemical similarity
suggest that this is not an infrequent scenario.
between butylene glycol and propylene glycol gives
Systemic androgen modulators provide an alternate
a high degree of confidence with regard to its poten-
treatment option for some of these patients.
tial for transcutaneous delivery of minoxidil. Despitethis chemical similarity, an immunologic distinction
REFERENCES
between the two solvents has been confirmed by
1. Olsen EA, editor. Disorders of hair growth diagnosis and treat-
previous patch test studies.19 However, in actual clin-
ical use, some patients whose patch tests were nega-
2. Scow DT, Nolte RS, Shaughnessy AF. Medical treatments for
tive to butylene glycol subsequently proved to be
balding in men. Am Fam Physician 1999;59:2189-94, 2196.
intolerant to the compounded preparation. This may
3. Walsh DS, Dunn CL, James WD. Improvement in androgenetic
alopecia (stage V) using topical minoxidil in a retinoid vehicle
be due to the inflamed state of their scalp, leaving it
and oral finasteride. Arch Dermatol 1995;131:1373-5.
more susceptible to further irritation. If, in fact,
4. Rogaine extra strength for men slide lecture kit. Pharmacia &
patients are found to be clinically intolerant to buty-
312 Brief reports
5. Price VH, Menefee E, Strauss PC. Changes in hair weight and hair
13. Ebner H, Muller E. Allergic contact dermatitis from minoxidil.
count in men with androgenetic alopecia, after application of
5% and 2% topical minoxidil, placebo, or no treatment. J Am
14. Alomar A, Smandia JA. Allergic contact dermatitis from minoxi-
dil. Contact Dermatitis 1988;18:51-2.
6. Catanzaro J, Smith G. Propylene glycol dermatitis. J Am Acad
15. Valsecchi R, Cainelli T. Allergic contact dermatitis from minoxi-
dil. Contact Dermatitis 1987;17:58-9.
7. Kinnunen T, Hannuksela M. Skin reactions to hexylene glycol.
16. van der Willigen AH, Dutree-Meulenberg RO, Stolz E, Geursen-
Reitsma AM, van Joost TH. Topical minoxidil sensitization in
8. Agren-Jonsson S, Magnusson B. Sensitization to propantheline
androgenic alopecia. Contact Dermatitis 1987;17:44-5.
bromide trichlorocarbanilide and propylene glycol in an
17. Tosti A, Bardazzi F, De Padova MP, Caponeri GM, Melino M,
antiperspirant. Contact Dermatitis 1976;2:79-80.
Veronesi S. Contact dermatitis to minoxidil. Contact Dermatitis
9. Warshaw TG, Herrmann F. Studies of skin reactions to propylene
glycol. J Invest Dermatol 1952;19:423-9.
18. Degreef H, Hendrickx I, Dooms-Goossens A. Allergic contact
10. Kosann MK, Brancaccio RR, Shupack JL, Franks AG Jr, Cohen DE.
dermatitis to minoxidil. Contact Dermatitis 1985;13:194-5.
Six-hour versus 48-hour patch testing with varying concentra-
19. Sugiura M, Hayakawa R. Contact dermatitis due to 1,3-butylene
tions of potassium dichromate. Am J Contact Dermatitis 1998;
glycol. Contact Dermatitis 1997;37:90-6.
20. Fisher AA. Use of glycerin in topical minoxidil solutions for
11. Cohen DE. Occupational dermatology. In: Harris RL, editor.
patients allergic to propylene glycol. Cutis 1990;45:81-2.
Patty’s Industrial hygiene. New York: John Wiley & Sons; 2000. p.
21. De George MS. Hair setting products. In: Rieger MM, editor.
Harry’s Cosmeticology. New York: Chemical Publishing Co;
12. Sanchez-Motilla J, Pont V, Nagore E, Rodriguez-Serna M,
Sanchez J, Aliaga A. Pustular allergic contact dermatitis fromminoxidil. Contact Dermatitis 1998;38:283-4.
Interoute Management Biographies Photos of the Interoute Management Team are also available for download from the website http://www.interoute.com/about-us/leadership. For additional information, please contact us: Interoute Communications Limited Walbrook Building 195 Marsh Wall London E14 9SG T +44 020 725 9000 E [email protected] W www.interoute.com Registered address as above
SINGAPORE: The Threat of Influenza Pandemic and Singapore’s Response Plan Pandemic Preparedness 1. Singapore has developed a pandemic preparedness plan detailing actions to be taken before and during an influenza pandemic. Our Influenza Pandemic Readiness and Response Plan was published and made available to the general public through MOH’s website in June 2005. The objective of the p
 310 Brief reports
310 Brief reports