Prevalence and correlates of premature ejaculation in a primary care setting: a preliminary crosssectional study
Prevalence and Correlates of Premature Ejaculation in a Primary Care Setting: A Preliminary Cross-Sectional Studyjsm_22801.8
Wei Shuong Tang, MMed* and Ee Ming Khoo, MD†
*Bayan Baru Health Clinic, Bayan Baru, Penang, Malaysia; †Department of Primary Care Medicine, University of Malaya,Kuala Lumpur, Malaysia
A B S T R A C T Introduction. Premature ejaculation (PE) is common. However, it has been underreported and undertreated. Aims. To determine the prevalence of PE and to investigate possible associated factors of PE. Methods. This cross-sectional study was conducted at a primary care clinic over a 3-month period in 2008. Men aged 18–70 years attending the clinic were recruited, and they completed self-administered questionnaires that included the Premature Ejaculation Diagnostic Tool (PEDT), International Index of Erectile Function, sociodemography, lifestyle, and medical illness. The operational definition of PE included PE and probable PE based on the PEDT. Main Outcome Measure. Prevalence of PE. Results. A total of 207 men were recruited with a response rate of 93.2%. There were 97 (46.9%) Malay, 57 (27.5%) Chinese, and 53 (25.6%) Indian, and their mean age was 46.0 Ϯ 12.7 years. The prevalence of PE was 40.6% (N = 82) (PE: 20.3%, probable PE: 20.3% using PEDT). A significant association was found between ethnicity and PE (Indian 49.1%, Malay 45.4%, and Chinese 24.6%; c2 = 8.564, d.f. = 2, P = 0.014). No significant association was found between age and PE. Multivariate analysis showed that erectile dysfunction (adjusted odds ratio [OR] 4.907, 95% confidence interval [CI] 2.271, 10.604), circumcision (adjusted OR 4.881, 95% CI 2.346, 10.153), sexual intercourse Յ5 times in 4 weeks (adjusted OR 3.733, 95% CI 1.847, 7.544), and Indian ethnicity (adjusted OR 3.323, 95% CI 1.489, 7.417) were predictors of PE. Conclusion. PE might be frequent in men attending primary care clinics. We found that erectile dysfunction, circumcision, Indian ethnicity, and frequency of sexual intercourse of Յ5 times per month were associated with PE. These associations need further confirmation. Tang WS and Khoo EM. Prevalence and correlates of premature ejaculation in a primary care setting: A preliminary cross-sectional study. J Sex Med **;**:**–**. Key Words. Patient-Reported Outcome Measures for Premature Ejaculation; Premature Ejaculation; Prevalence; Primary Health Care Introduction
The DSM-IV-TR [6] defines PE as “a persis-
tent or recurrent ejaculation with minimal sexual
P remature ejaculation (PE) is a common male stimulationbefore,on,orshortlyafterpenetration
sexual dysfunction. The prevalence ranged
and before the person wishes it and it causes
between 21% and 66% in the community [1–3]
marked distress or interpersonal difficulty and is
not due to the direct effects of a substance.”
Various definitions have been used to define PE,
Currently, there are five validated tools that are
and these include: the Diagnostic and Statistical
used to assess PE: the five-item Premature Ejacu-
Manual of Mental Disorders, Fourth Edition, Test
lation Diagnostic Tool (PEDT) [9,10]; the Prema-
Revision (DSM-IV-TR) [6]; the 10th revision of
ture Ejaculation Profile [11], which used the
the International Classification of Diseases-10 [7];
DSM-IV-TR classification criteria; the 10-item
and the evidence-based definition from the Inter-
Chinese Index of Premature Ejaculation [12],
national Society for Sexual Medicine [8].
which was developed as an efficacy measure but
2011 International Society for Sexual Medicine
did not specifically address the DSM-IV-TR cri-
stress, the options were “a lot,” “somewhat,”
teria; the Arabic questionnaires [13]; and the Index
of Premature Ejaculation [14]. Among these tools,
The PEDT consists of five questions that
the PEDT was found to have a high level of agree-
address the following five domains: ejaculation
ment with the clinical diagnosis, and its test–retest
control; frequency of PE; ejaculation with minimal
reliability was good with an intraclass correlation
sexual stimulation; distress; and interpersonal dif-
ficulty. Each question has five responses, and the
PE is associated with age, lifestyle [16], and
scores of each question range from 0 to 4 with a
comorbidities such as depression [17], anxiety
minimum total score of 0 to a maximum score of
[17,18], social phobia [19,20], diabetes [21], pros-
20. A low score suggests a low probability of
tate diseases [22–24], and erectile dysfunction (ED)
having PE. The total scores are categorized into:
[25]. Despite PE being common, very few studies
“no PE” (Յ8), “probable PE” (9–10), and “PE”
have been conducted in the primary care setting.
(Ն11). In our study, the operational definition of
This study aimed to determine the prevalence of
PE included “PE” and “probable PE.”
PE using PEDT and to identify possible associated
Two versions of PEDT were used: the original
factors of PE among primary care clinic attendees.
English version and the translated Malay ver-sion. The PEDT was translated into the Malaylanguage using the forward and backward transla-
tion process, and it was done independently
We conducted a cross-sectional study in the
by two postgraduate family medicine trainees who
primary care clinic at the University Malaya
are bilingual. The back-translated English version
Medical Center (UMMC), which is a teaching
was compared with the original English version,
university hospital in Kuala Lumpur, Malaysia.
and further revisions were made. The final Malay
Ethics approval was obtained from the UMMC
version of the PEDT was sent to the copyright
Medical Ethics Committee prior to commence-
owner for approval to be used in the study.
A convenience sampling method was used.
having attempted sexual intercourse in the past 4
weeks [26]. Therefore, in this study, the IIEF-5
between June and August 2008 were approached
was completed only by participants who had
and recruited in this study. The reasons for
sexual intercourse in the past 4 weeks. Men who
encounter were chronic disease follow-up; treat-
did not have sexual intercourse in the past 4
ment for acute conditions such as infection or
weeks were asked to self-report whether they
injury; and undifferentiated problems. They
have ED. The operational definition of ED in
might or might not have men’s health issues. The
this study included men with IIEF-5 scores of
inclusion criteria were: all men aged 18–70 years
(Malaysian national language); had experience of
A pilot study was conducted with 15 men, and
sexual intercourse; and were currently not taking
the questionnaires were pretested. Minimal adjust-
a selective serotonin reuptake inhibitor. Informed
ment was made. The sample size was calculated
consent was obtained from those who agreed to
using Epi Info version 6 (Centers for Disease
participate in the study. The participants were
Control and Prevention, Atlanta, GA, USA). Based
asked to complete a set of self-administered ques-
on an estimated PE prevalence of 30% with 95%
tionnaires in English or Malay language, and
confidence interval and taking into account a
they consisted of: questions on sociodemography,
refusal rate of 20%, the estimated sample size was
lifestyle, medical conditions, and sexual history;
International Index of Erectile Function-5 (IIEF-
Data were analyzed using the SPSS 15.0 (SPSS
5); and PEDT. The participants were asked to
Inc., Chicago, IL, USA) software [27]. Chi-square
self-report whether they had any of the following
test was used to determine the associations
between categorical variables. The significance
demia, diabetes mellitus, prostate disease, insom-
level (a) was set at 0.05. Odds ratio was calculated
nia, depression, and anxiety. For question on
to examine the strength of the associations. Mul-
exercise, the participants were given options of
tivariate analysis was used to examine the net effect
“never,” “<4 times/month,” “1–3 times/week,” or
of independent variables on PE and to determine
“Ն4 times/week,” while for the question on
Premature Ejaculation and Associated Factors
Background sociodemographic characteristics,
health, lifestyle, and sexual behavior of the respondent
A total of 245 men were approached to participatein the study, of which 222 patients fulfilled
the inclusion criteria and 207 men consented. Theresponse rate was 93.2%. The mean age of the
participants was 46.0 Ϯ 12.7 years, and the major-
ity was Malays followed by Chinese and Indians.
The majority of the respondents were employed,
married, and sexually active. Most respondents
had sexual intercourse in the last 4 weeks. The
majority had average to very high libido, and the
5.2 Ϯ 5.4 per 4 weeks (see Table 1). Based on the
IIEF-5, 127 (61.4%) men had ED. Forty (19.3%)
patients who did not have sexual intercourse in the
past 4 weeks were asked to answer the question on
self-reported ED; 17 of the 40 (42.5%) men self-
reported ED. In this study, ED included men with
reported ED, with an overall prevalence of 69.6%.
The prevalence of PE using the study opera-
tional definition was 40.6% (N = 84) (probable PE
[N = 42, 20.3%] and PE [N = 42, 20.3%] based on
the PEDT). No significant association was found
between PE and age groups (c2 = 1.406, d.f. = 4,
PE was found to be significantly associated
with ethnicity, circumcision, ED, and frequency
of sexual intercourse using univariate analysis
(Table 2). Using binary logistic regression (back-
ward logistic regression [LR] method), ED, cir-
cumcision, sexual intercourse (Յ5 times per 4
weeks), and Indian ethnicity were predictive factors
Discussion
Sexual intercourse within last 4 weeks 167 (80.7)Libido/sexual interest
Using the study operational definition, the preva-
lence of PE among men who attended a teaching
hospital-based primary care clinic was 40.6%.
This was consistent with the findings from other
studies, which reported the prevalence of PE
ranging from 21% to 66% [1–3], including a study
done in a Malaysia urban population where the
prevalence of self-reported PE was 22.3% [16]. We included “probable PE” from the PEDT inthe operational definition as it is known that men
Indian ethnicity was found to be significantly
underreport their sexual problems and do not seek
associated with PE. The multi-country concept
medical help [28]. If the “PE” category alone was
evaluation and assessment of PE incidence study
examined, the prevalence of 20.3% was consistent
have shown substantial geographical variation in
with the findings of self-reported PE in the previ-
the perception of how long it takes for the
ous study [16]. It is likely the probable PE category
“average” man to ejaculate [29]. The difference in
of the PEDT was mild and was not perceived by
perception of normal intravaginal ejaculatory
latency time (IELT) may cause difference in per-
Figure 1 Prevalence
ejaculation according to age groups.
ception of poor control of ejaculation and related
mechanism of this relationship is yet to be charac-
distress, and hence the problem of PE. These
terized but may include reduced performance
variations could be because of differences in reli-
anxiety, a higher ejaculatory threshold, or superior
gion, awareness of sexual dysfunction, ability to
ejaculatory control because of earlier and superior
admit sexual failure, and cultural perception on the
recognition of prodromal ejaculatory sensations.
importance of sex [30]. This ethnic difference
Among the medical illnesses, ED was the only
requires further studies for confirmation.
condition that had shown a significant association
We found that circumcision was independently
with PE. This corresponded with the Jannini et al.
associated with PE. This finding was consistent
study that found that ED may be a comorbid, a
with the O’Hara and O’Hara study [31], where
cause, or an effect of PE [25]. Many men may find
women reported that their circumcised male
it confusing to differentiate between PE and ED,
partners were more likely to have PE than the
as was demonstrated in the Global of Study of
uncircumcised partners. The thickening and kera-
Sexual Attitudes and Behaviors [1]. It is therefore
tinization of the glans penis mucosal epithelium
important to further evaluate these conditions as
after circumcision may be responsible for the dif-
ference in the sensory threshold of the glans penis.
No significant association was found between
The nerves of the glandis corona may be hyper-
age and PE. This finding was similar to that found
stimulated during intercourse and hence trigger
in the PE Prevalence and Attitudes survey [3] and
ejaculation before it is desired [32]. However,
the prevalence study of sexual dysfunction in the
there were prospective studies [33,34] that exam-
United States [2]. The prevalence of PE is similar
ined sexual function before and after circumcision,
across the age groups, while the prevalence of ED
and found that circumcision did not appear to have
increases with age [38,39]. Anxiety and depression
an adverse effect. Waldinger et al. [29] also did not
were not found to be significantly associated with
find any significant difference in the median IELT
PE in the study as was noted in others’ studies
between circumcised and not circumcised men in
[16,17]. This may be because of the small number
five countries excluding Turkey. Further studies
of respondents with anxiety and depression in this
study. In addition, the self-reported dichotomous
Frequency of sexual intercourse of Յ5 times in
scale of “yes” or “no” response for these conditions
4 weeks was also found to be significantly associ-
may not reflect the prevalence of the disease.
ated with PE. It is likely that men with PE would
This study was limited by enrolling patients
have less sexual intercourse, or it could also be
who understood either English or the Malay lan-
plausible that infrequent sexual intercourse con-
guage. However, as this study was done at an urban
tributed to PE. The relationship between ejacula-
tertiary hospital, most patients were literate in
Malay or English. Nevertheless, this study could
intercourse is conflicting. While the study of Jang
be further improved if other languages such as
[35] and Spiess et al. [36] reported that the fre-
Tamil and Mandarin versions of the questionnaires
quency of sexual activity in men with PE was
are made available in this multicultural society.
lower than age-matched controls with normal
This study was also limited by its cross-sectional
ejaculatory control, in contrast, Strassberg et al.
design, and it was conducted in a hospital-based
[37] failed to demonstrate any relationship. The
primary care practice. Thus, the findings may not
Premature Ejaculation and Associated Factors
Associated factors of premature ejaculation
PE = premature ejaculation; OR = odds ratio; CI = confidence interval; BMI = body mass index.
be generalizable. However, it provides an insight
PE and need treatment in the long term. In addi-
to this condition in the primary care setting, which
tion, studies using the latest evidence-based defi-
was lacking. A longitudinal study can be done for
nition of PE by the International Society for
men with probable PE to evaluate if they develop
Sexual Medicine Committee [40] can be used in
Independent associated factors of PE using multiple logistic regression
PE = premature ejaculation; SE = standard error; OR = odds ratio; CI = confidence interval.
the primary care setting to further evaluate this
Bayan Baru, George Town, Penang 11950, Malaysia.
common male sexual dysfunction. PE is defined as
“a male sexual dysfunction characterized by ejacu-
lation which always occurs prior to or within about
one minute of vaginal penetration, and the inabil-ity to delay ejaculation on all or nearly all vaginalpenetrations,
Statement of Authorship
quences.” Studies have indicated that patients’ or
partner’s self-reported ejaculatory latency time
(a) Conception and Design
correlates relatively well with the objective stop-
watch latency time [40–42]. Thus, patients and/or
(b) Acquisition of Data
their partners with probable PE and PE can be
further evaluated based on their self-reported
(c) Analysis and Interpretation of Data
IELT rather than the stopwatch latency time. The
self-reported IELT is more applicable in theprimary care settings and can help primary care
physicians to decide on the treatment plan [43]. (a) Drafting the Article
Dapoxetine, an on-demand short-acting serotonin
selective reuptake inhibitor, has been shown to
(b) Revising It for Intellectual Content
improve the IELT and can be used to treat PE[44–46]. Category 3 (a) Final Approval of the Completed Article Conclusion
PE might be a common male sexual dysfunction inprimary care clinic attendees. It was found to be
References
independently associated with ED, circumcision,
1 Laumann EO, Nicolosi A, Glasser DB, Paik A, Gingell C,
Indian ethnicity, and frequency of sexual inter-
Moreira E, Wang T. Sexual problems among women and men
course in this study. It is therefore important to
aged 40–80 y: Prevalence and correlates identified in the
assess PE in men presenting with ED. Moreover,
Global Study of Sexual Attitudes and Behaviors. Int J Impot
physicians, especially the primary care physicians,
2 Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the
who provide first-contact care must be aware of
this common condition in men. Primary care phy-
sicians need to be trained to detect, diagnose, and
3 Porst H, Montorsi F, Rosen RC, Gaynor L, Grupe S, Alex-
ander J. The Premature Ejaculation Prevalence and Attitudes
(PEPA) survey: Prevalence, comorbidities, and professionalhelp-seeking. Eur Urol 2007;51:816–24. Acknowledgments
4 Read S, King M, Watson J. Sexual dysfunction in primary
medical care: Prevalence, characteristics and detection by the
The authors would like to thank Professor Low Wah
general practitioner. J Public Health Med 1997;19:387–91.
Yun, Associate Professor Dr. Ng Chirk Jenn, and Miss
5 Aschka C, Himmel W, Ittner E, Kochen MM. Sexual prob-
lems of male patients in family practice. J Fam Pract
Mahanim for their comments and suggestion in this
6 American Psychiatric Association. Diagnostic and statistical
manual of mental disorders. 4th edition. Text revision: DSM-
Corresponding Author: Wei Shuong Tang, MMed,
IV-TR. Washington, DC: American Psychiatric Association;
Klinik Kesihatan Bayan Baru, Primary Care, 11950
Premature Ejaculation and Associated Factors
7 WHO. International statistical classification of diseases and
26 Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Pena BM.
related health problems. Tenth Revision. Geneva, Switzerland:
Development and evaluation of an abridged, 5-item version of
the International Index of Erectile Function (IIEF-5) as a diag-
8 McMahon CG, Althof S, Waldinger MD, Porst H, Dean J,
nostic tool for erectile dysfunction. Int J Impot Res
Sharlip I, Adaikan PG, Becher E, Broderick GA, Buvat J,
Dabees K, Giraldi A, Giuliano F, Hellstrom WJG, Incrocci L,
27 Statistical Package for Social Sciences. SPSS for Windows
Lean E, Meuleman E, Perelman MA, Rosen R, Rowland D,
version 15. Chicago, IL: SPSS Inc.; 2006.
Segraves R. An evidence-based definition of lifelong
28 White AK. Men and the problem of help seeking. In: Heidel-
premature ejaculation: Report of the International Society
baugh JJ, ed. Clinical men’s health: Evidence in practice.
for Sexual Medicine (ISSM) ad hoc committee for the
Philadelphia, PA: Elsevier; 2007:31–44.
definition of premature ejaculation. BJU Int 2008;102:338–50.
29 Waldinger MD, Quinn P, Dilleen M, Mundayat R, Schweitzer
9 Symonds T, Perelman MA, Althof S, Giuliano F, Martin M,
DH, Boolell M. A multinational population survey of intrav-
May K, Abraham L, Crossland A, Morris M. Development and
aginal ejaculation latency time. J Sex Med 2005;2:492–7.
validation of a premature ejaculation diagnostic tool. Eur Urol
30 Jannini EA, Lenzi A. Epidemiology of premature ejaculation.
10 Kam SC, Han DH, Lee SW. The diagnostic value of the
31 O’Hara K, O’Hara J. The effect of male circumcision on the
premature ejaculation diagnostic tool and its association with
sexual enjoyment of the female partner. BJU Int 1999;83(suppl
intravaginal ejaculatory latency time. J Sex Med 2011;8:865–71.
11 Patrick DL, Giuliano F, Ho KF, Gagnon DD, McNulty P,
32 Kim D, Pang M. The effect of male circumcision on sexuality.
Rothman M. The Premature Ejaculation Profile: Validation of
self-reported outcome measures for research and practice. BJU
33 Senkul T, Iseri C, Sen B, Karademir K, Saracoglu F, Erden D.
Circumcision in adults: Effect on sexual function. Urology
12 Yuan YM, Xin ZC, Jiang H, Guo YJ, Liu WJ, Tian L, Zhu JC.
Sexual function of premature ejaculation patients assayed with
34 Collins S, Upshaw J, Rutchik S, Ohannessian C, Ortenberg J,
Chinese Index of Premature Ejaculation. Asian J Androl
Albertsen P. Effects of circumcision on male sexual function:
Debunking a myth? J Urol 2002;167:2111–2.
13 Arafa M, Shamloul R. Development and evaluation of the
35 Jang SY. Korean study for the relationship between premature
Arabic Index of Premature Ejaculation (AIPE). J Sex Med
ejaculation and frequency of sexual intercourse. J Mens Health
14 Althof S, Rosen R, Symonds T, Mundayat R, May K, Abraham
36 Spiess WF, Geer JH, O’donohue WT. Premature ejaculation:
L. Development and validation of a new questionnaire to assess
Investigation of factors in ejaculatory latency. J Abnorm
sexual satisfaction, control, and distress associated with prema-
ture ejaculation. J Sex Med 2006;3:465–75.
37 Strassberg DS, Kelly MP, Carroll C, Kircher JC. The psycho-
15 Symonds T, Perelman M, Althof S, Giuliano F, Martin M,
physiological nature of premature ejaculation. Arch Sex Behav
Abraham L, Crossland A, Morris M, May K. Further evidence
of the reliability and validity of the premature ejaculation diag-
38 Blanker HM, Bosch JL, Groeneveld FP, Bohnen AM, Prins A,
nostic tool. Int J Impot Res 2007;19:521–5.
Thomas S, Hop WC. Erectile and ejaculatory dysfunction in a
16 Schiavi RC, Stimmel BB, Mandeli J, White D. Chronic alco-
community-based sample of men 50 to 78 years old: Preva-
lence, concern, and relation to sexual activity. Urology
17 Quek KF, Sallam AA, Ng CH, Chua CB. Prevalence of sexual
39 Nicolosi A, Glasser DB, Moreira ED, Villa M. Prevalence of
problems and its association with social, psychological and
erectile dysfunction and associated factors among men without
physical factors among men in a Malaysian population: A
concomitant diseases: A population study. Int J Impot Res
cross-sectional study. J Sex Med 2008;5:70–6.
18 Strassberg DS, Brazao CA, Rowland DL, Tan P, Slob AK.
40 Rosen R, Sadovsky R, Becher E, Brodevick GA, Buvat J, Gold-
Clomipramine in the treatment of rapid (premature)
stein I, EL-Meliery AI, Giuliano F, Hellstrom WJG, Incrocci
ejaculation. J Sex Marital Ther 1999;25:89–101.
L, Jannini EA, Park K, Parrish S, Porst H, Rowland D, Seg-
19 Tignol J, Martin-Guehl C, Aouizerate B, Grabot D, Auria-
raves R, Sharlip I, Simonelli C, Tan HM. International Society
combe M. Social phobia and premature ejaculation: A
for Sexual Medicine’s guidelines for the diagnosis and treat-
case-control study. Depress Anxiety 2006;23:153–7.
ment of premature ejaculation. J Sex Med 2010;7:2947–
20 Corretti G, Pierucci S, De Scisciolo M, Nisita C. Comorbidity
between social phobia and premature ejaculation: Study on 242
41 Althof SE. Evidence based assessment of rapid ejaculation. Int
males affected by sexual disorders. J Sex Marital Ther
J Impot Res 1998;10(suppl 2):S74–6.
42 Rosen RC, McMahon CG, Niederberger C, Broderick GA,
21 El-Sakka AI. Premature ejaculation in non-insulin-dependent
Jamieson C, Gagnon DD. Correlates to the clinical diagnosis
diabetic patients. Int J Androl 2003;26:329–34.
of premature ejaculation: Results from a large observa-
22 Mulligan T, Retchin SM, Chinchilli VM, Bettinger CB. The
tional study of men and their partners. J Urol 2007;177:1059–
role of aging and chronic disease in sexual dysfunction. J Am
43 McMahon CG. Clinical trial methodology in premature
23 Screponi E, Carosa E, Di Stasi SM, Pepe M, Carruba G,
ejaculation observational, interventional, and treatment
Jannini EA. Prevalence of chronic prostatitis in men with pre-
preference studies—Part II—Study design, outcome measures,
mature ejaculation. Urology 2001;58:198–202.
data analysis, and reporting. J Sex Med 2008;5:1817–33.
24 Shamloul R, el-Nashaar A. Chronic prostatitis in premature
44 Porst H, McMahon CG, Althof SE, Sharlip I, Bull S, Aquilina
ejaculation: A cohort study in 153 men. J Sex Med
JW, Tesfaye F, Rivas DA. Baseline characteristics and treat-
ment outcomes for men with acquired or lifelong premature
25 Jannini EA, Lombardo F, Lenzi A. Correlation between ejacu-
ejaculation with mild or no erectile dysfunction: Integrated
latory and erectile dysfunction. Int J Androl 2005;28(suppl
analyses of two phase 3 dapoxetine trials. J Sex Med
45 Althof SE, Brock GB, Rosen RC, Rowland DL, Aquilina JW,
46 McMahon CG, Althof SE, Kaufman JM, Buvat J, Levine SB,
Rothman M, Tesfaye F, Bull S. Validity of the patient-
Aquilina JW, Tesfaye F, Rothman M, Rivas DA, Porst H.
reported Clinical Global Impression of Change as a
Efficacy and safety of dapoxetine for the treatment of prema-
measure of treatment response in men with premature
ture ejaculation: Integrated analysis of results from five phase 3
ejaculation. J Sex Med 2010;7:2243–52.
What does hormone imbalance mean and how can it affect me? Pre-menstrual syndrome (PMS), irregular menses, infertility, fibrocystic breasts, uterine fibroids and menopause are representative of women’s health conditions that are caused by an imbalance in hormones. Causes can include exogenous estrogens; chemicals found in food, air and water; malfunctions in liver detox pathways and stres
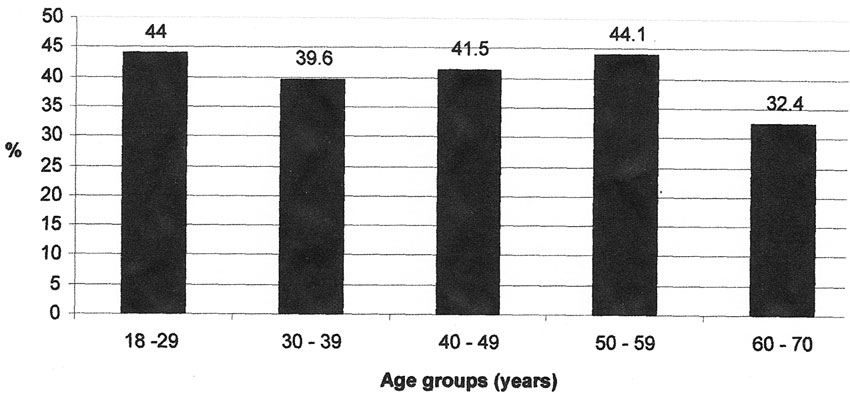 Figure 1 Prevalence
Figure 1 Prevalence