1499 BOARDMAN-CANFIELD RD BOARDMAN, OH 44512 WEBSITE: WWW.YOUNGSTOWNORTH.COM
IMPORTANT INFORMATION: PLEASE BRING TO YOUR SCHEDULED APPOINTMENT ANY AND ALL FILMS (XRAYS, MRI, BONE SCAN, ETC) THAT YOU MAY HAVE HAD DONE. FAILURE TO DO THIS MAY CAUSE YOUR APPOINTMENT TO BE RESCHEDULED. CANCELLATIONS MUST BE MADE 24 HOURS IN ADVANCE OF THE SCHEDULED APPOINTMENT OR YOA RESERVES THE RIGHT TO ASSESS A FEE OF $25.00. COPAYS ARE DUE AT THE TIME OF VISIT. PLEASE PRINT AND FILL OUT PAPERWORK IN IT’S ENTIRETY AND RETURN TO YOA 5 DAYS PRIOR TO SCHEDULED VISIT.
FAMILY PHYSICIAN:________________________REFERRING PHYSICIAN:_______________________ PATIENTS LEGAL NAME:__________________________________________DATE: ______/______/_____ STREET,CITY,STATE,ZIP:___________________________________________________________________ SS#:________/________/________ DATE OF BIRTH:_______/______/______ AGE:________
LEFT HANDED RIGHT HANDED IS YOUR PROBLEM RELATED TO (CHECK ONE): ACCIDENT DATE PROBLEM OCCURRED: _________/________/________ PLEASE BRIEFLY DESCRIBE YOUR MAIN PROBLEM/COMPLAINT _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ HOW LONG HAVE YOU HAD THIS PROBLEM? ________________________________
WHAT POSITION(S)/ACTIVITIES MAKE THE PAIN WORSE OR BETTER? ACTIVITY WORSE BETTER BOWEL MOVEMENT COUGHING GENERAL ACTIVITY HOME REMEDY LYING DOWN STANDING HOW LONG CAN YOU STAND WITH MINIMAL OR NO PAIN (IN MINUTES)?_________________
WALKING DISTANCE WITH MINIMAL OR NO PAIN (CHECK BOX) 50-200 FT. 200-500 FT. DO YOU NEED ASSISTANCE TO HELP YOU WALK? IF YES, WHAT TYPE OF SUPPORT?_____________________________________________________________ DO YOU WEAR A BACK OR NECK BRACE? IF YES, HOW LONG?__________________________________________________________________________ PHYSICIAN SIGNATURE:______________________________________________DATE:____________________________
LIST ALL THE PREVIOUS DOCTORS (MD, DO, CHIROPRACTOR) YOU HAVE SEEN FOR YOUR MAIN COMPLAINT PHYSICIAN SPECIALTY TREATMENT INDICATE WHICH DIAGNOSTIC TESTS YOU HAVE HAD TO EVALUATE YOUR MAIN COMPLAINT PLAIN X-RAY EMG/NCV/SSEP BONE SCAN ARTHROGRAM MYELOGRAM DEXA SCAN DISKOGRAM LIST ALL TREATMENTS YOU HAVE HAD PRIOR TO TODAY THAT ARE RELATIVE TO YOUR CONDITION TREATMENT HELPFUL? ELECTRICAL STIMULATION TENS UNIT ULTRASOUND HOT PACKS COLD PACKS WHIRLPOOL POOL EXERCISES HOME EXERCISES MANIPULATION ACUPUNCTURE INJECTIONS PHYSICIAN SIGNATURE:______________________________________________DATE:____________________________
1499 BOARDMAN-CANFIELD RD BOARDMAN, OH 44512 WEBSITE: WWW.YOUNGSTOWNORTH.COM
IMPORTANT INFORMATION: PLEASE BRING TO YOUR SCHEDULED APPOINTMENT ANY AND ALL FILMS (XRAYS, MRI, BONE SCAN, ETC) THAT YOU MAY HAVE HAD DONE. FAILURE TO DO THIS MAY CAUSE YOUR APPOINTMENT TO BE RESCHEDULED. CANCELLATIONS MUST BE MADE 24 HOURS IN ADVANCE OF THE SCHEDULED APPOINTMENT OR YOA RESERVES THE RIGHT TO ASSESS A FEE OF $25.00. COPAYS ARE DUE AT THE TIME OF VISIT. PLEASE PRINT AND FILL OUT PAPERWORK IN IT’S ENTIRETY AND RETURN TO YOA 5 DAYS PRIOR TO SCHEDULED VISIT.
PATIENTS LEGAL NAME:__________________________________________ PAST MEDICAL HISTORY HAVE YOU HAD ANY OF THE FOLLOWING? –CHECK ALL THAT APPLY COMMENTS COMMENTS BOWEL DISORDERS CANCER (WHERE) PSORIASIS DEPRESSION RHEUMATISM DIABETES SEIZURES HEART DISEASE SERIOUS INFECTION HIGH BLOOD PRESSURE KIDNEY DISEASE LUNG DISEASE MULTIPLE MYELOMA PACEMAKER SURGICAL HISTORY PLEASE LIST ANY SURGERY (S) YOU HAVE HAD BY TYPE, DATE AND OUTCOME: ARE YOU ALLERGIC TO ANY MEDICATION (S)? NO IF YES, WHAT TYPE OF REACTION (S)? MEDICATION: REACTION: MEDICATION: REACTION: MEDICATION: REACTION: LATEX ALLERGIES: TOBACCO USE NO IF YES, AGE/YEAR STARTED: _________ YEAR QUIT:____________ PLEASE INDICATE QUANTITY PER DAY OF THE FOLLOWING CIGARETTES CHEWING TOBACCO (SNUFF) ALCOHOL USE NO IF YES, AGE/YEAR STARTED: _________ YEAR QUIT:____________ PLEASE INDICATE QUANTITY PER DAY OF THE FOLLOWING: DISTILLED SPIRITS HAVE YOU EVER BEEN TREATED FOR DRUG OR ALCOHOL ADDICTION? PHYSICIAN SIGNATURE:______________________________________________DATE:____________________________
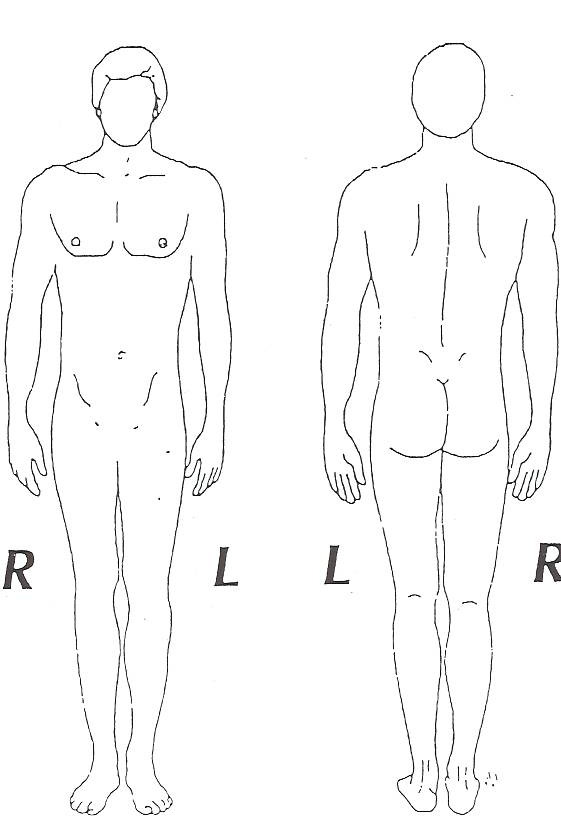
PATIENTS LEGAL NAME:__________________________________________ USING THE SYMBOLS BELOW, PLEASE DRAW IN THE LOCATION OF YOUR SYMPTOMS ON THE DIAGRAMS. FRONT BACK XXXX PAIN 0000 NUMBNESS ____________________________________________________ PAIN SCALE: 0 1 2 3 4 5 6 7 8 9 10 MARK AN (X) ON THE LINE INDICATING THE USUAL DEGREE OF THE PAIN (0 = NO PAIN, 10 = THE WORST PAIN IN YOUR LIFE, i.e. toothache, labor pain, kidney stone(s),etc. IF YOU HAVE NECK PAIN, WHAT PERCENTAGE OF YOUR PAIN IS_______% NECK ________% ARM=100% IF YOU HAVE BACK PAIN, WHAT PERCENTAGE OF YOUR PAIN IS_______% BACK ________% LEG=100% PHYSICIAN SIGNATURE:______________________________________________DATE:____________________________
1499 BOARDMAN-CANFIELD RD BOARDMAN, OH 44512 WEBSITE: WWW.YOUNGSTOWNORTH.COM
IMPORTANT INFORMATION: PLEASE BRING TO YOUR SCHEDULED APPOINTMENT ANY AND ALL FILMS (XRAYS, MRI, BONE SCAN, ETC) THAT YOU MAY HAVE HAD DONE. FAILURE TO DO THIS MAY CAUSE YOUR APPOINTMENT TO BE RESCHEDULED. CANCELLATIONS MUST BE MADE 24 HOURS IN ADVANCE OF THE SCHEDULED APPOINTMENT OR YOA RESERVES THE RIGHT TO ASSESS A FEE OF $25.00. COPAYS ARE DUE AT THE TIME OF VISIT. PLEASE PRINT AND FILL OUT PAPERWORK IN IT’S ENTIRETY AND RETURN TO YOA 5 DAYS PRIOR TO SCHEDULED VISIT.
PATIENTS LEGAL NAME:__________________________________________ PLEASE LIST ALL MEDICATIONS YOU ARE TAKING MEDICATION DOSE: (MG.MCG) TIMES PER DAY HOW LONG? HAVE YOU PREVIOUSLY TAKEN ANY OF THESE DRUGS? SKELAXIN CLINORIL MECLOMEN DARVOCET NAPROSYN TOLECTIN DILAUDID DISALCID PARAFON FORTE TYLENOL #3 PERCODAN PREDNISONE FELEDENE FLEXERIL VOLTAREN IBUPROFIN WORKING STATUS FULL DUTY LIGHT DUTY OFF DUTY PER DR. EMPLOYED UNEMPLOYED IF NOT FULL DUTY: HOW LONG HAVE YOU BEEN OFF WORK? HAVE YOU HAD A WORK CAPACITY ASSESSMENT? ARE YOU DISABLED THROUGH SOCIAL SECURITY?
MENTAL HEALTH HAVE YOU/OR ARE YOU SEEING A DOCTOR FOR MENTAL ILLNESS: IF YES, WITH WHOM? FOR WHAT REASON? MEDICATION(S): PHYSICIAN SIGNATURE:______________________________________________DATE:____________________________ PATIENTS LEGAL NAME:__________________________________________ PHYSIC REVIEW OF SYSTEMS PLEASE CHECK IF YOU HAVE EXPERIENCED ANY OF THE FOLLOWING WEIGHT GAIN LAST 6 MONTHS WEIGHT LOSS LAST 6 MONTHS NIGHT SWEATS BLEED EASILY ANY RASHES BRUISE EASILY RECENT CHANGE IN VISION RECENT CHANGE IN SMELL DIZZINESS RECENT CHANGE IN HEARING RECENT CHANGE IN TASE SHORTNESS OF BREATH WHEEZING HISTORY OF TUBERCULOSIS CHEST PAIN SHORTNESS OF BREATH FEET EDEMA (SWELLING) WITH EXERCISE PALPITATIONS HEART MURMUR PACE MAKER DIARRHEA ABDOMINAL PAIN VOMITING INDIGESTION BLOODY OR DARK STOOLS BLOOD IN URINE UNABLE TO CONTROL BLADDER RUSHING TO GO URINARY TRACT INFECTION UNABLE TO CONTROL BOWEL NEED TO GO FREQUENTLY ATTACK OF WEAKNESS JOINT PAIN/SWELLING /MORNING STIFFNESS POOR APPETITE NUMBNESS/TINGLING FEET CRYING SPELLS PROBLEM SLEEPING NUMBNESS/TINGLING HANDS CONVULSIONS
FEMALE – PLEASE WRITE IN DATE IF APPROPRIATE ABNORMAL VAGINAL BLEEDING HISTORY OF BREAST BIOPSY HISTORY OF NIPPLE DISCHARGE HISTORY OF ENDOMETRIOSIS LAST MENSTRUAL PERIOD
MALE – PLEASE WRITE IN DATE IF APPROPRIATE HISTORY OF PROSTATITIS DIFFCULTY URINATING LAST PROSTATIC EXAM RECTAL EXAM RESULTS: PSA (PROSTATE BLOOD TEST) RESULTS: DESCRIBE CURRENT HEALTH, AGE, CAUSE OF DEATH, ILLNESS, DIABETES, CANCER, HYPERTENSION, ETC. DECEASED MEDICAL HISTORY/CAUSE OF DEATH SIBLING (1) SIBLING (2) SIBLING (3) PATIENT SIGNATURE:______________________________________ DATE: ______/______/_____
1499 BOARDMAN-CANFIELD RD BOARDMAN, OH 44512 WEBSITE: WWW.YOUNGSTOWNORTH.COM
IMPORTANT INFORMATION: PLEASE BRING TO YOUR SCHEDULED APPOINTMENT ANY AND ALL FILMS (XRAYS, MRI, BONE SCAN, ETC) THAT YOU MAY HAVE HAD DONE. FAILURE TO DO THIS MAY CAUSE YOUR APPOINTMENT TO BE RESCHEDULED. CANCELLATIONS MUST BE MADE 24 HOURS IN ADVANCE OF THE SCHEDULED APPOINTMENT OR YOA RESERVES THE RIGHT TO ASSESS A FEE OF $25.00. COPAYS ARE DUE AT THE TIME OF VISIT. PLEASE PRINT AND FILL OUT PAPERWORK IN IT’S ENTIRETY AND RETURN TO YOA 5 DAYS PRIOR TO SCHEDULED VISIT. LEGAL FULL NAME:_________________________________________________________________DATE:_____/_____/_____ PHONE NUMBER WE CAN REACH YOU OTHER THAN YOUR HOME TELEPHONE NUMBER: CELL PHONE #:___________________ WORK PHONE:___________________________ OCCUPATION:_________________________________ EMPLOYER:_________________________________ YEARS THERE:____ EMPLOYERS STREET/CITY/STATE/ZIP:________________________________________________________________ NAME OF SPOUSE (IF APPLICABLE:)______________________________________BIRTHDATE:__________AGE:________ OCCUPATION:______________________EMPLOYER:__________________________________________ YEARS THERE:_____ EMPLOYERS STREET/CITY/STATE/ZIP:_________________________________________________________________________ MAY WE CONTACT HIM/HER AT WORK? YES IF YES, PHONE NUMBER/EXT. ___________________ IN CASE OF EMERGENCY, WHO CAN WE CONTACT OUTSIDE OF YOUR HOUSEHOLD ? NAME:________________________________________ RELATIONSHIP:_____________________________________________ PHONE #:________________ CAN WE USE CELL #? YES I F YES, CELL# __________________________ __________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
FOR MINOR OR POWER OF ATTORNEY RESPONSIBLE PARTY:______________________________________RELATIONSHIP TO PATIENT:___________________________ SS#:____/____/____ BIRTHDATE:___/____/____ AGE: ___ STREET/PO BOX:_____________________________CITY:_________________________________ST:______ ZIP:__________ TELEPHONE NUMBER:______________________ CELL PHONE NO.:_________________________ OCCUPATION:_____________EMPLOYER:______________________________ YEARS THERE:______ EMPLOYERS STREET/CITY/STATE/ZIP:_________________________________________________________________________
MAY WE CONTACT HIM/HER AT WORK? YES IF YES, PHONE NUMBER/EXT. ___________________ _______________________________________________________________________________________________________________________________________________________________________________________ DO YOU WISH YOUR PHONE CALLS TO BE CONFIDENTIAL?
IS THIS VISIT DUE TO A WORK RELATED INJURY OR PROBLEM?
IF YES, ON WHAT DATE DID THE INJURY OR PROBLEM OCCUR ________CLAIM NO.__________________ DID YOU REPORT THE ACCIDENT TO YOUR EMPLOYER? WAS THIS THE RESULT OF AN AUTO ACCIDENT? YES
IF YES, DATE OF THE ACCIDENT____________ IS SOMEONE ELSE FINANCIALLY LIABLE FOR YOUR INJURY?
PRIMARY INSURANCE – NAME OF INSURANCE COMPANY: INSURANCE ADDRESS (STREET/CITY/STATE/ZIP):
INSURED’S NAME: INSURED’S DATE OF BIRTH: EMPLOYER POLICY/ID #: GROUP. NO.:
SECONDARY INSURANCE – NAME OF INSURANCE COMPANY:
INSURANCE ADDRESS (STREET/CITY/STATE/ZIP):
INSURED’S NAME: INSURED’S DATE OF BIRTH: EMPLOYER:
ACTA PHILOSOPHICA, vol. 4 (1995), fasc. 2 - PAGG. 137-147 “Orexis”, “Telos” y “Physis” Un comentario con ocasión de EN 1094a l9ss * 1. Propósito En Etica Nicomaquea I, 2, 1094a 19ss, Aristóteles se aboca a mostrar que en elobrar humano existe un fin óptimo, cuyo conocimiento se requiere para una vida plena. El propósito de este escrito es analizar el argumento aducid
NIMH · What medications are used to treat anxiety disorders?http://www.nimh.nih.gov/health/publications/mental-health-medication. Back to: NIMH Home » Health Topics » Publications » Mental Health MedicationsWhat medications are used to treat anxiety disorders?Read Publication on Single Page | Table of ContentsPrevious Page: What medications are used to treat bipolar disorder?Ne
 PATIENTS LEGAL NAME:__________________________________________
PATIENTS LEGAL NAME:__________________________________________