Hoang Thu Vu,* Katrin C. Leitmeyer,†1 Dang Ha Le,‡ Megge J. Miller,§1 Quang Hien Nguyen,‡1 Timothy M. Uyeki,¶1 Mary G. Reynolds,¶1 Jesper Aagesen,#1 Karl G. Nicholson,**1 Quang Huy Vu,* Huy Anh Bach,††1 and Aileen J. Plant‡‡1
We investigated the clinical manifestations and course
tries had reported 8,098 probable cases of SARS and 774
of all probable severe acute respiratory syndrome (SARS)
patients in the Vietnam outbreak. Probable SARS cases
Coronavirus was first hypothesized to be the etiologic
were defined by using the revised World Health
agent of SARS by Peiris et al. (3). Later, two independent
Organization criteria. We systematically reviewed medical
teams (4,5) confirmed the novel coronavirus was associat-
records and undertook descriptive statistical analyses. All
ed with SARS infections in patients from Hong Kong,
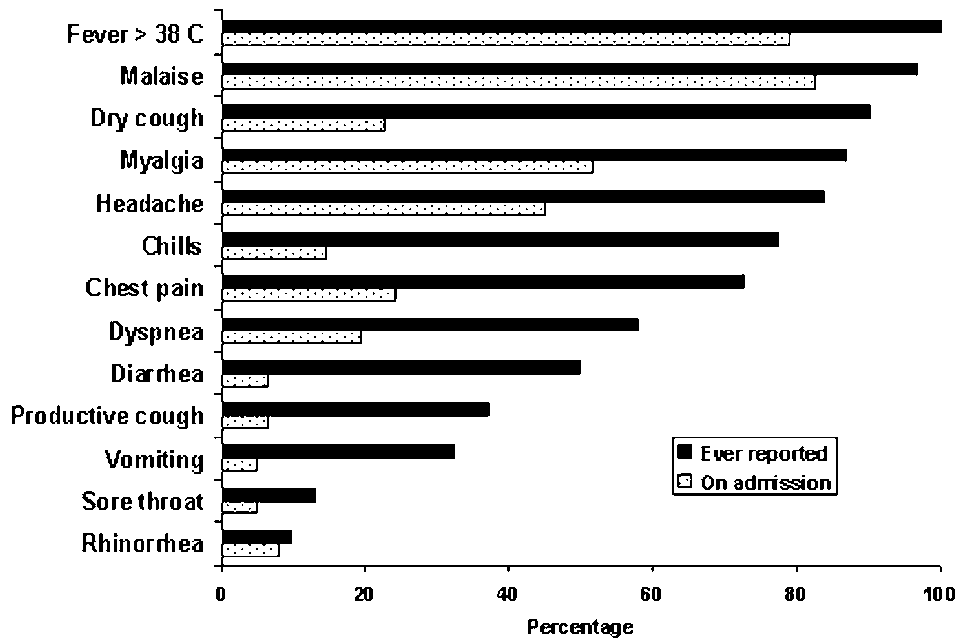
62 patients were hospitalized. On admission, the mostprominent symptoms were malaise (82.3%) and fever
Vietnam, Canada, and Taiwan. This article describes the
(79.0%). Cough, chest pain, and shortness of breath were
clinical and laboratory features of patients with SARS in
present in approximately one quarter of the patients; 79.0%
had lymphopenia; 40.3% had thrombocytopenia; 19.4%had leukopenia; and 75.8% showed changes on chest radi-
ograph. Fever developed on the first day of illness onset,and both respiratory symptoms and radiographic changes
Case Definition and Ascertainment
occurred on day 4. On average, maximal radiographic
We used the World Health Organization (WHO) case
changes were observed on day 10, and fevers subsided by
definition (April 1 revision) for SARS in this investigation
day 13. Symptoms on admission were nonspecific,although fever, malaise, and lymphopenia were common.
(6). A probable case-patient was defined as a person who
The complications of SARS included invasive intubation
sought treatment after November 1, 2002, with a high
and ventilation (11.3%) and death (9.7%).
fever (>38°C) and cough or breathing difficulty and infil-trates shown on chest radiograph consistent with pneumo-nia or respiratory distress syndrome. A probable case-
The global outbreak of severe acute respiratory syn- patient was excluded if an alternative reason could fully
drome (SARS) has been epidemiologically linked to
explain the illness, e.g., proven tuberculosis or clinical
an outbreak that is believed to have begun during
response within 48 hours to antibacterial therapy. For prac-
November 2002 in Guangdong Province, People’s
tical purposes, we modified the case definition to only
Republic of China (1). SARS then spread to other coun-
include cases occurring on or after February 23, the date of
tries and regions, such as the Hong Kong Special
onset of symptoms of the Vietnam index case. Serologic
Administrative Region of China, Vietnam, Singapore,
testing for SARS-associated coronavirus (SARS-CoV)
Canada, and Taiwan. By the end of the outbreak, 26 coun-
was performed on serum specimens as previouslydescribed (4).
*Hanoi French Hospital, Hanoi, Vietnam; †Robert-Koch Institut,
Case-patients were identified by clinicians, and consid-
Berlin, Germany, and World Health Organization, Geneva,
erable effort was made by the Vietnam Ministry of Health
Switzerland; ‡Bach Mai Hospital, Hanoi, Vietnam; §Australian
to train both metropolitan and rural staff in surveillance
National University and Commonwealth Department of Health andAgeing, Canberra, Australia; ¶Centers for Disease Control and
and identification of SARS. Many case-patients were
Prevention, Atlanta, Georgia, USA; #Swedish Institute for
admitted to hospital with suspected SARS; however, only
Infectious Disease Control, Jonkoping, Sweden; **Leicester RoyalInfirmary, Leicester, United Kingdom; ††Hanoi Medical University,Hanoi Vietnam; and ‡‡Curtin University of Technology, Perth,
1Members of the World Health Organization SARS Team in
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 10, No. 2, February 2004
those whose condition conformed to the WHO case defini-tion are included in this analysis.
The medical records of SARS case-patients were retro-
spectively reviewed by physicians. We used a standard-ized data collection form to record patient information. For the nine patients admitted to the hospital after March20, clinical data were collected prospectively. For eachcase-patient, clinical signs, symptoms, radiologic find-ings, and data from biochemical, hematologic, and micro-biologic tests throughout the course of illness wererecorded. When assessing the proportion of case-patientswith symptoms, if the information about a symptom wasnot recorded, we assumed the symptom did not occur. Forthe hematologic and biochemical course of illness, all
Figure 1. Symptoms of patients with probable severe acute respi-
available measurements were used, with recordings for
ratory syndrome (N = 62), at hospital admission and reported dur-
>15 case-patients per day, and the measurements are dis-
ing the course of illness, Vietnam, February–May 2003. Note: Allcase-patients had fever during their illness because this was part
played with accompanying standard deviation of means.
Onset of illness was defined as the date when each case-patient first reported feeling unwell with symptoms com-
the patients had symptoms of the lower respiratory tract on
admission; dry cough (22.6%), chest pain (24.2%), anddyspnea (19.4%). The proportion of patients who reported
Data Analysis
dry cough at any time throughout the illness increased to
Data from the medical records were entered into
90.3%. Other lower respiratory tract symptoms also
Microsoft Excel and analyzed with Epi-Info version 6 soft-
became more prominent after admission. Upper respirato-
ware. We analyzed the data by using standard descriptive
ry tract symptoms were reported infrequently.
statistical techniques. To describe the course of the illness,the maximum temperature, leukocyte count, platelet count
and lymphocyte count data from every case were com-
Fever was present at admission for 79.0% of case-
bined and averaged for each day of the illness.
patients, with 66.1% having fever >38°C, although, as perthe case definition, all case-patients experienced fever dur-
ing their illness. Crepitations were present on admission in
The first SARS case-patient in Vietnam was admitted to
35.5% of patients, and in 87.1%, crepitations developed
the hospital on February 26, 2003, and the last case-patient
during the course of their illness. On admission, 47 (75.8%)
was admitted on April 8, 2003. All 62 patients with proba-
patients had abnormal chest radiographic results. The radi-
ble SARS were admitted to hospitals in Hanoi, Vietnam.
ographs of the remaining 15 case-patients showed abnor-
The initial case-patients were admitted to a small private
malities 2 to 7 days (median 5) from the admission date.
hospital (hospital A), and the later case-patients were
On admission, the radiographic changes were mainly
admitted to a facility at a large public hospital, hospital B.
interstitial infiltrates, bilateral or unilateral, affecting less
Of the 62 case-patients, 61 (98.4%) were seropositive for
than two thirds of the lungs. Maximal radiographic
SARS-CoV. The number of case-patients who were sus-
changes during the illness were mainly bilateral interstitial
pected of having SARS but later excluded is not known.
infiltrates or bilateral alveolar opacities affecting morethan two thirds of both lungs. The degree of change on the
Study Population
chest radiograph did not always appear to correlate with
The mean age of SARS patients was 40.8 years (medi-
the apparent severity of illness as defined by the need for
an 43, range 20–76 years) and 39 (62.9%) were female. A
detailed description of the epidemiology of the SARS out-
The mean white blood cell count on admission was
break in Vietnam will be published separately.
5.9 x 109/L, ranging between 2.7 and 16.3 x 109/L (Table). Leukopenia was found in 19.4% of patients, and lym-
Clinical Features
phopenia occurred in 79.3% of case-patients on admission,with lymphopenia defined as total lymphocyte count
Symptoms
below 1.5 x 109 /L. Thrombocytopenia was observed in
The most prominent symptoms on admission were
40.3% of patients on admission, with a mean platelet count
malaise and myalgia (Figure 1). Less than one quarter of
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 10, No. 2, February 2004
Table. Hematologic and biochemical features of patients with severe acute respiratory syndrome on admission
Twenty-seven of the patients had biochemical blood
We observed that the time from symptom onset to admis-
tests performed. For these patients, 34.5% had elevated
sion decreased during the outbreak (data not shown).
alanine aminotransferase levels, and 42.9% had abnormal-ly high levels of aspartate aminotransferase. We observed
Case Management
hyponatremia in 29.6% of patients on admission, and14.8% of patients had hypokalemia. Respiratory Therapy Respiratory assistance was required for 38 (61.2%) of Natural History of Illness
the patients: 25 (40.3%) patients required the use of sup-
The average maximum temperature for all of the case-
plemental oxygen; 6 (9.7%) required positive pressure
patients on day 1 of onset was 38.7°C and reached a max-
noninvasive ventilation while an additional 7 (11.3%)
imum of 39.0°C on day 5 (Figure 2). We observed that
patients were intubated and received mechanical ventila-
fever in SARS patients subsided on day 13. Overall, the
tion. Only 1 of the 7 who were intubated recovered.
average leukocyte count of all the cases never decreasedbelow 4.0 × 109/L, suggesting that leukopenia was not a
Antibiotics
common feature of SARS among the whole cohort, but did
A wide range of antibiotics were prescribed for SARS
occur in a few patients, as indicated by the error bars on
patients in Vietnam, including beta-lactams, tetracyclines,
Figure 2. Thrombocytopenia (platelet count < 150 × 109/L)
aminoglycosides, macrolides, and fluoroquinolones.
was present in the cohort from day 4 until day 9 of the ill-
Antibiotic therapy was not observed to be clinically bene-
ness. After day 10, the average platelet count returned to
within the normal range. Lymphopenia (lymphocyte count<1.5 × 109/L) was present throughout the course of the ill-
Antivirals
ness, with lymphocyte counts ranging from 1.0 to 1.5 ×
Patients in the first wave of the outbreak of SARS were
initially treated with oseltamivir when the etiologic agent
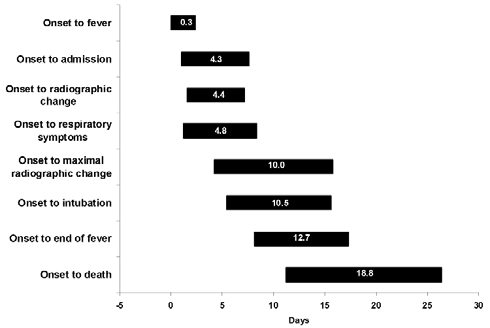
The natural history of SARS in Vietnam is shown in
was thought to be an influenza virus. Eighteen patients
Figure 3. Not all patients felt feverish at onset, but fever
(29.0%) received oral or intravenous ribavirin for an aver-
developed an average of 0.3 days after the onset of other
age of 9 days (median 12 days) after the onset of illness.
SARS symptoms. We observed that the average length of
Neither oseltamivir nor ribavirin was observed to have any
time from onset to observed radiographic changes and
clinically beneficial effect on the course of illness.
from onset to first respiratory symptoms were similar(4.4–4.8 days) and generally coincided with admission to
Steroids
hospital. Maximal radiographic changes occurred on the
For 14 patients, steroid treatment was begun an average
10th day of illness, on average, 3 days before fever sub-
of 8.2 days after the onset of illness (median 7 days).
sided. SARS patients were in hospital for, on average, 24.5
Patients were given steroids for a mean duration of 7.6
days (± 7.4 days). A total of six (9.7%) case-patients died.
days (range 1–14 days). No particular protocol existed for
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 10, No. 2, February 2004
Lymphopenia was constant throughout the illness and
thrombocytopenia, on average, lasted for 5 days, begin-ning on the fourth day after onset. Respiratory symptomsand the first radiographic changes were first noted on day4 of the illness. Maximal radiograph change generallyoccurred on day 10.
On admission, 6.5% of patients reported having diar-
rhea. However, patients with SARS may have recalled res-piratory symptoms more frequently than gastrointestinalsymptoms. During the full course of illness, half of theprobable SARS case-patients reported diarrhea. What pro-portion of these patients had diarrhea directly related toSARS or in response to antibiotic treatment is not known. Diarrhea, regardless of its cause, has important implica-tions for transmission of SARS, because SARS-CoV canbe shed in feces (10). However, it is not yet known whetherviable organisms are shed in quantities sufficient to consti-tute a substantial source for transmission. The role of diar-rhea in SARS transmission requires further investigation.
Our data on clinical symptoms at admission may not be
generalizeable to other SARS outbreaks for several rea-sons. Admission bias may have occurred at hospital A afterthe initial cluster among healthcare workers was recog-nized. In some instances, temperatures were being takenand some patients were admitted after fever onset but noother symptoms, daily chest x-rays were taken for somecase-patients, and some patients refused admission untilafter they had been ill for several days.
Microbiologic evaluation of patients who met the case
Figure 2. Average (±1 standard deviation) maximal daily tempera-
definition for probable SARS in Vietnam was difficult at
ture, leukocyte count, platelet count, and lymphocyte count by day
the time of admission. Decisions about case status on
of severe acute respiratory syndrome from onset, Vietnam,February–May 2003, (N = 62 cases but not for each data point).
admission were initially made by considering clinical signsand symptoms. We did not have laboratory facilities to con-
the timing or dosage of steroids given, making interpreta-
firm SARS, and facilities to identify other agents causing
atypical pneumonia were limited. Patients were treatedwith antibiotics for atypical bacterial pneumonia on admis-
Discussion
This is the first report of a complete outbreak of SARS
and as such includes all patients in whom SARS was diag-nosed from the beginning of the outbreak until SARS wasdeclared contained in Vietnam on April 28, 2003. Dr CarloUrbani (deceased), a public health physician with WHO inVietnam, first described the outbreak in reports to WHO atthe beginning of March 2003. He reported a similar pres-entation of case-patients that we describe. The main clini-cal features of probable SARS case-patients reported inVietnam were fever, malaise, dry cough, and infiltrates onradiographs. These findings are consistent with thosereported in Hong Kong (3,7), Singapore (8), and Canada. (9) Additionally, we have described the clinical develop-ment of SARS over time. The main feature exhibited by
Figure 3. Average (±1 standard deviation) duration of time from
SARS case-patients on hospital admission was fever,
onset of illness until outcome in the evolution of severe acute res-
which typically lasted 13–14 days after onset.
piratory syndrome, Vietnam, February–May 2003
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 10, No. 2, February 2004
sion to hospital, and if the patients responded to treatment
and the Tropical Medicine Institute at Bach Mai Hospital. Lastly,
within 48 hours, the SARS case status was revised.
we acknowledge the patients with SARS and their families.
All case-patients with probable SARS in the Vietnam
Dr. Vu is a clinical immunoallergist and was the primary cli-
outbreak were epidemiologically linked, and 98.4% had
nician looking after the SARS patients at hospital A. Since the
serologic evidence of SARS-CoV infection. After the ini-
outbreak of SARS, Dr. Vu has been involved in a range of
tial case, all probable SARS cases identified in the
Vietnam outbreak were among healthcare workers or closecontacts of case-patients.
Our findings in regard to treatment are nonspecific. References
Proven treatment options must await proper clinical trials
1. Centers for Disease Control and Prevention. Update: Outbreak of
severe acute respiratory syndrome—worldwide, 2003. Morb Mortal
Despite the nonspecific nature of SARS at clinical pres-
entation, a typical case had fever, myalgia, malaise fol-
2. World Health Organization. Cumulative number of reported probable
cases of severe acute respiratory syndrome (SARS). URL:
lowed several days later by cough and respiratory symp-
http://www.who.int/csr/sars/country/table2003_09_23/en/
toms. At this point the patient typically had changes shown
3. Peiris JSM, Lai ST, Poon LLM, Guan G, Yam LY, Lim W, et al.
by chest x-ray, lymphopenia, and thrombocytopenia. Due
Coronavirus as possible cause of severe acute respiratory syndrome.
to the nonspecific nature of SARS, both on admission and
4. Ksiazek TG, Erdman D, Goldsmith CS, Zaki SR, Peret T, Emery S, et
throughout the course of illness, clinicians must obtain a
al. A novel coronavirus associated with severe acute respiratory syn-
detailed exposure history for anyone presenting with atyp-
drome. N Engl J Med 2003; 348:1953–66.
ical pneumonia to help in the early diagnosis and manage-
5. Drosten C, Gunther S, Preiser W, van der Werf S, Brodt HR, Becker
ment of a potential outbreak situation. When the diagnosis
S, et al. Identification of a novel coronavirus in patients with severeacute respiratory syndrome. N Engl J Med 2003: May 15;348:
is in doubt, the person should be isolated under strict infec-
tion control procedures until the diagnosis becomes clear.
6. Global surveillance for severe acute respiratory syndrome. Wkly
Acknowledgments
7. Lee N, Hui D, Wu A, Chan P, Cameron P, Joynt GM, et al. A major
outbreak of severe acute respiratory syndrome in Hong Kong. N Engl
We dedicate this paper to the late Dr. Carlo Urbani, who pro-
vided the first epidemiologic and clinical descriptions of SARS
8. Hsu L-Y, Le C-C, Green JA, Ang B, Patton NI, Lee L, et al. Severe
and died from SARS as a result of his early investigation.
acute respiratory syndrome (SARS) in Singapore: clinical features ofindex patient and initial contacts. Emerg Infect Dis 2003;9:713–7.
We thank the Ministry of Health, Vietnam, for support of our
9. Poutanen SM, Low DE, Henry B, Finkelstein S, Rose D, Green K, et
efforts, especially Minister of Health Tran Thi Trung Chien, Vice
al. Identification of severe acute respiratory syndrome in Canada. N
Minister of Health and Chair of the SARS Taskforce Nguyen Van
10. World Health Organization. Severe acute respiratory syndrome—
Thuong, Le Thi Thu Ha, and the many persons in the Ministry of
multi-country outbreak-update 47: Studies of SARS virus survival,
Health who assisted us. We also thank Pascale Brudon, Rodger
situation in China. [cited 2003 May 7] Available from: URL:
Doran, Helen-Louise Taylor, the WHO staff in Vietnam, and
http://www.who.int/csr/don/2003_05_05/en/
other members of the WHO SARS team in Vietnam, Manila, andGeneva; Nguyen Ngoc Tho and J. Gouzee, who provided clinical
Address for correspondence: A.J. Plant, Division of Health Sciences,
care to the patients; and the staff of the Ha Noi French Hospital
Curtin University of Technology, GPO Box U1987 Perth, Western
Australia 6845; fax: +61 8 9266 2608; email: [email protected]
The editors of Emerging Infectious Diseases seek to increase the roster of reviewers for manuscripts submitted by authors all
over the world for publication in the journal. If you are interested in reviewing articles on emerging infectious disease topics,please e-mail your name, address, curriculum vitae, and areas of expertise to [email protected]
At Emerging Infectious Diseases, we always request reviewers’ consent before sending manuscripts, limit review requests to
three or four per year, and allow 2-4 weeks for completion of reviews. We consider reviewers invaluable in the process of select-ing and publishing high-quality scientific articles and acknowledge their contributions in the journal once a year.
Even though it brings no financial compensation, participation in the peer-review process is not without rewards. Manuscript
review provides scientists at all stages of their career opportunities for professional growth by familiarizing them with researchtrends and the latest work in the field of infectious diseases and by improving their own skills for presenting scientific informa-tion through constructive criticism of those of their peers. To view the spectrum of articles we publish, information for authors,and our extensive style guide, visit the journal web site at www.cdc.gov/eid.
For more information on participating in the peer-review process of Emerging Infectious Diseases, e-mail
[email protected] or call the journal office at 404-371-5329.
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 10, No. 2, February 2004
Prof. Dr méd. Stefan Zeuzem Hépatite B Risques, prévention et traitement European Liver Patients Association F. De Renesselaan, 57B - 3800 Sint-Truiden, Belgium email: [email protected] Cette brochure doit vous aider à en savoir plus sur votremaladie et et à mieux vivre avec. Elle doit vous encoura-ger à maintenir un mode de vie normal avec vos sembla-bles et ne pas développe
Data Roaming Service Coverage and Tariff Updated Since 10 Oct 2013 Minimum Charge Unit Thereafter Charge Destination Network Code Charges (HK$/KB) Unit (KB) 收費 ( 港幣 $/KB) Data Roaming Service Coverage and Tariff Updated Since 10 Oct 2013 Minimum Charge Unit Thereafter Charge Destination Network Code Charges (HK$/KB) Unit (KB) 收�
 those whose condition conformed to the WHO case defini-tion are included in this analysis.
those whose condition conformed to the WHO case defini-tion are included in this analysis.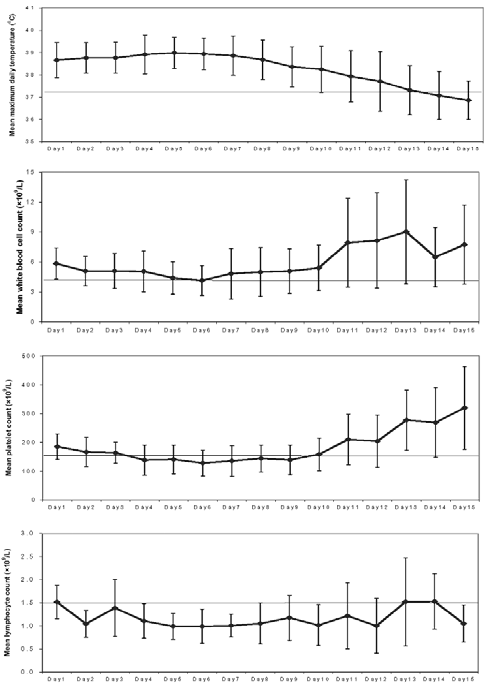
 Lymphopenia was constant throughout the illness and
thrombocytopenia, on average, lasted for 5 days, begin-ning on the fourth day after onset. Respiratory symptomsand the first radiographic changes were first noted on day4 of the illness. Maximal radiograph change generallyoccurred on day 10.
On admission, 6.5% of patients reported having diar-
rhea. However, patients with SARS may have recalled res-piratory symptoms more frequently than gastrointestinalsymptoms. During the full course of illness, half of theprobable SARS case-patients reported diarrhea. What pro-portion of these patients had diarrhea directly related toSARS or in response to antibiotic treatment is not known.
Lymphopenia was constant throughout the illness and
thrombocytopenia, on average, lasted for 5 days, begin-ning on the fourth day after onset. Respiratory symptomsand the first radiographic changes were first noted on day4 of the illness. Maximal radiograph change generallyoccurred on day 10.
On admission, 6.5% of patients reported having diar-
rhea. However, patients with SARS may have recalled res-piratory symptoms more frequently than gastrointestinalsymptoms. During the full course of illness, half of theprobable SARS case-patients reported diarrhea. What pro-portion of these patients had diarrhea directly related toSARS or in response to antibiotic treatment is not known.