RBMOnline - Vol 7. No 2. 194–199 Reproductive BioMedicine Online; www.rbmonline.com/Article/894 on web 16 June 2003
Premature LH and progesterone rise inintrauterine insemination cycles: analysis ofrelated factors
João Sabino Cunha-Filho obtained his MD degree (1993) and the speciality degree inObstetrics and Gynecology (1997) at the Faculty of Medicine (Hospital de Clínicas de PortoAlegre, Universidade Federal do Rio Grande do Sul) in Brazil. The PhD degree was grantedto him at the same University in 2000. He continued with post-doctoral studies at Clamart,France (2001). At present he is Professor in Obstetrics and Gynaecology at the Faculty ofMedicine–Hospital de Clínicas de Porto Alegre in Brazil and has authored more than 150publications in national and international journals and books. His current research interestsinclude assisted reproduction, endometriosis and ovarian stimulation.
João Sabino Cunha-Filho, Jacques Kadoch, Claudia Righini, Renato Fanchin, René Frydman, François Olivennes1Service de Gynécologie-Obstétrique et Biologie de la ReproductionHôpital Antoine Béclère, Clamart, France1Correspondence: Service de Gynécologie Obstétrique, Hôpital Cochin Saint-Vincent-De-Paul, 27 rue du FaubourgSaint Jacques, 75679 Paris Cedex 14, France. Tel +33 1 58411555; Fax +33 1 58411539; e-mail:[email protected]
Premature LH and progesterone surges are associated with different factors and hormonal modulators. The aim of thepresent study was (i) to investigate the clinical and laboratory factors and (ii) to highlight the importance of differentstimulation protocols in associated premature LH and progesterone surges in intrauterine insemination (IUI) cycles. Thestudy involved a retrospective investigation of 75 patients undergoing IUI for infertility treatment (135 IUI cycles) between1996 and 2000, with initial serum LH concentrations >10 mIU/ml during ovarian stimulation. Ultrasound characteristics,follicular sizes, serum oestradiol, progesterone and LH concentrations and ovarian stimulation protocols were measured. There was a wide range of oestradiol serum concentrations (93–2245 pg/ml) and follicular size (12–25 mm). In 49.6% ofcycles, the dominant follicle was <16.5 mm. Patients with >2 follicles measuring <15 mm had higher oestradiol serumconcentrations (P = 0.008). Multiple regression analyses revealed no association between these variables and prematureLH/progesterone surge. In conclusion, LH/progesterone surges cannot be predicted utilizing clinical parameters normallyemployed, e.g. ultrasound serum oestradiol assay or ovarian stimulation protocol. Patients with follicles >14 mm or moreand with high numbers of small follicles and high oestradiol are at risk of a spontaneous LH surge. These variables can beused to time the administration of GnRH antagonist administration until better predictive factors are demonstrated. Keywords: intrauterine insemination, LH rise, premature luteinization, progesterone increase
in IVF to avoid cycle cancellations, which occur in 25% ofcases (Eibschitz et al., 1986). In addition, this rise is a good
The determination of LH surge and its associated factors is a
predictor of LH surge and ovulation. In stimulated cycles,
controversial issue. Published papers differ in studied
small follicles may release more oestradiol, increasing the risk
populations, outcomes and statistical models. Moreover, the
of premature LH rise (Testart and Frydman, 1982). Moreover,
modulation of LH surge by oestradiol is disputed by several
other factors may be equally important for LH regulation
authors (Eibschitz et al., 1986; Kreiner et al., 1988; Couzinet
(Loumaye, 1990), since even seasonal and diurnal LH
and Schaison, 1993; Taylor et al., 1995). Others describe an
variability cannot be explained by steroid serum
association between maximum follicular size and LH surges
concentrations alone (Testart et al., 1982). The importance of
(Eissa et al., 1986), and propose a role for gonadotrophin surge-
progesterone support on different stimulation regimes
attenuating factor (GnSAF) in these events (Fowler et al., 1993).
(Macnamee et al., 1988) shows the significance of lutealprogesterone secretion and ovarian stimulation on results
Predicting the initial LH rise during the LH surge is mandatory
Article - Premature LH and progesterone rise in IUI - JS Cunha-Filho et al
Many of these physiological events were determined and
studied 20 years ago, using the more limited technologies ofultrasound and hormone assays, when recombinant FSH,
gonadotrophin-releasing hormone (GnRH) agonists andantagonists were not available. GnRH antagonists were
A retrospective analysis was carried out of all cases of IUI
recently introduced for IVF–embryo transfer, and probably for
intrauterine insemination (IUI) also. Two regimens have beendescribed, single- and multiple-dose protocols (Alabano et al.,
1997; Olivennes et al., 1998; Borm and Mannaerts, 2000). Both regimens can be used in a fixed schedule, in which the
A total of 135 cycles were analysed among 75 patients
antagonist is injected on a particular day of the stimulation
admitted for IUI at Hôpital Antoine Béclère, Clamart, who
cycle. A more flexible approach would be possible if the
showed a spontaneous LH surge during ovarian stimulation or
antagonist could be administered only when an LH rise is
spontaneous cycles between 1996 and 2000.
feared, perhaps diminishing the dose of antagonist or evenidentifying patients for whom antagonists are unnecessary. To
IUI was used for treatment of infertility, and stimulation
prescribe such protocols, parameters are needed to predict the
protocols were prescribed according to clinical factors. The
initial LH rise to screen patients at risk of premature
various protocols included spontaneous cycles using
clomiphene, short agonist, human menopausal gonadotrophin(HMG) and recombinant (rec)FSH.
This new understanding of ovarian cycle and folliculardevelopment, and the advent of several protocols for ovarian
stimulation, including the introduction of recombinant FSH,led to the analysis of the impact of new regimens on LH
After day 8 of the, cycle, patients were assessed by measuring
surges. A reappraisal of common parameters could be useful
oestradiol, LH and progesterone in serum, and using
when combined with new computerized technology for
transvaginal ultrasound to assess follicular development.
hormonal assays (e.g. chemoluminescence) and the wideutilization of transvaginal ultrasound, with better probes of
Spontaneous LH surges were considered in patients presenting
higher frequency and increased accuracy of diagnostic
with serum LH concentrations >10 IU/l during the stimulation
equipment (De Boever et al., 1983; Freimanis and Jones,
protocol, and serum progesterone concentrations >1 ng/ml,
1992; Hershlag et al., 2000).
according to Fanchin et al. (1996).
The present study thus aims to analyse clinical and laboratory
The number of days required for ovulation induction, together
data in different ovarian stimulation protocols in relation to
with serum LH, progesterone and oestradiol on the day of the
spontaneous elevated serum LH concentrations in patients
LH rise, were analysed. Oestradiol output per follicle was
measured as a marker of oestradiol secretion related tofollicular development.
Numbers of follicles >12 mm, diameters of dominant folliclesand total numbers of follicles were assessed. Table 1. Comparison of stimulation duration, steroid concentrations and follicle sizes using the different stimulation protocols (medians and ranges).
aP < 0.05 in comparison with other groups.
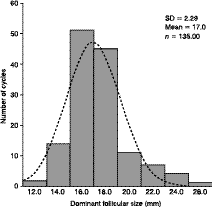
Article - Premature LH and progesterone rise in IUI - JS Cunha-Filho et alFigure 1. Distribution of surges of dominant follicles (mm) and the normal (Gaussian) distribution curve (dotted line).
Patients with >10 follicles at the onset of stimulation protocolwere considered to have a polycystic ovary (PCO)-like profile. Follicle diameters were measured by two differentinvestigators, using transvaginal ultrasound (7.5 MHztransvaginal probe; Siemens Elegra®; Siemens SAS, Saint-Denis, France) and calculated as the mean of twoperpendicular measures.
Plasma oestradiol, progesterone, LH and FSH concentrationswere determined by automated and direct chemoluminescentmethods (ACS:180; Chiron Diagnostics Corp., USA). Sensitivity (minimum detectable concentration) was 10 pg/mlfor oestradiol (conversion factor to SI units, 3.671), 0.1 ng/mlfor progesterone (conversion factor 3.180), 0.1 mIU/ml for LH(conversion factor 1.00) and 0.3 mIU/ml for FSH (conversionfactor 1.00). Intra- and inter-assay coefficients of variation
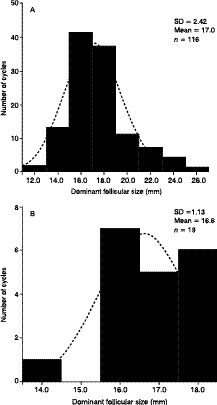
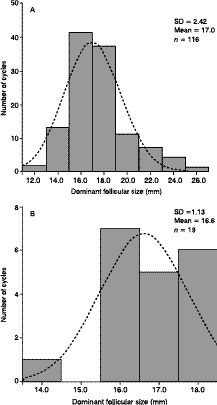
Figure 2. Distribution of sizes of dominant follicles size (mm)
over the concentration range were <7% for oestradiol, <10%
and normal (Gaussian) distribution curve (dotted line) in
for progesterone and <5% for both LH and FSH.
patients with stimulated cycles (A) and spontaneous cycles (B), P > 0.05.
The groups were divided according the prescribed stimulation
protocol. To compare studied variables among the groups,Kruskall–Wallis or Mann–Whitney U-tests were used, since
Table 1 shows the results for ovarian stimulation with different
the distribution of data was not parametric.
protocols. A total of 75 patients (median age 33 years; range25–41) were studied in 135 cycles. The most important
The effect on premature luteinization as the dependent
findings included the wide range observed for oestradiol serum
variable, assessed by serum LH concentrations >10 IU/l and
concentrations (median: 437.50 pg/ml; range: 93–2245 pg/ml)
progesterone >1 ng/ml, was measured using multiple
and dominant follicular size (median and mean: 17.00 mm;
regressions in two models. The first model assessed the impact
range: 12–25 mm; SD: 2.29, coefficient of variability:
of the stimulation protocol to elicit premature luteinization.
The second model utilized age, dose of gonadotrophins (IU),total number of follicles >12 mm, serum oestradiol
Patients on spontaneous cycles showed an LH surge at lower
concentrations, size of dominant follicle and PCO-like ovarian
serum oestradiol concentrations than in stimulated patients,
profile as independent variables. All variables are expressed as
medians and ranges. The significance level was 5%.
Distributions in the sizes of dominant follicules are shown in
Figures 1 and 2. Dominant follicles in 67 patients (49.6%)
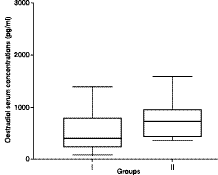
Article - Premature LH and progesterone rise in IUI - JS Cunha-Filho et alTable 2. Multiple regression analysis (dependent variable: serum progesterone concentration >1 ng/ml). Model 1: independent variable: ovarian stimulation protocolsModel 2: independent variable: clinical and laboratory data.Figure 3. Distribution of serum oestradiol concentrations
(pg/ml). The box represents the interquartile range which
contains 50% of the values. The whiskers are lines extending
from the box to the highest and lowest values, excluding
outliers. A line across the box indicates the median. Group I
comprises patients with follicles >15 mm (n = 114) and group
II those with >2 follicles <15 mm (n = 21) (P = 0.008).
were <16.5 mm. Normal distribution curves of dominant
follicles. Moreover, during spontaneous cycles, the initial LH
rise is elicited in a different manner than in stimulated cycles.
Overall differences between the sizes of dominant follicles in
In addition, a particular group of patients with a large number
spontaneous and stimulated cycles did not differ (Figure 2).
of follicles <15 mm in diameter had higher concentrations ofserum oestradiol and were at risk of premature luteinization.
Multiple logistic regression analyses were applied toinvestigate possible factors associated with precocious rises in
Oestradiol is essential for oocyte development and the LH
surge. However, the critical limit when serum oestradiol
concentrations >1 ng/ml were the dependent variable
concentrations elicit these rapid LH releases is controversial
(premature luteinization) in two different models. In model 1,
(Kreiner et al., 1988; Cahill et al., 1998, 2000). Some authors
five different ovarian stimulation protocols were investigated
propose that rapid rises in concentrations of oestradiol are
as the independent variable. In model 2, independent variables
more important than serum concentrations per se (Kreiner et
included age, dose of gonadotrophins (IU), serum oestradiol
al., 1988). Others show how only 1% of infertile patients with
concentrations, PCO-like profiles, total number of follicles
tubal occlusion begin their LH surge with serum oestradiol
and size of the dominant follicle (Table 2). The occurrence of
concentrations <600 pmol/l (Cahill et al., 1998).
premature luteinization was not associated with any of theseindependent variables.
Our multiple regression analysis clearly confirms that LHsecretion is not solely under the influence of dominant
The impact of small follicles on hormonal serum
follicular size, numbers of follicles or concentrations of
concentrations was assessed by comparing cycles with >2
steroids in serum, as found by other groups (Loumaye, 1990;
follicles measuring <15 mm [group I (n = 21)] versus those
Kagawa et al., 1992; Couzinet and Schaison, 1993; Fowler et
with follicles measuring >15 mm [group II (n = 114)]. This
al., 1993; Costello et al., 1998; McCartney et al., 2002).
analysis shows that patients with >2 follicles measuring <15mm had higher oestradiol serum concentrations (P = 0.008,
Other ovarian factors may be necessary to modulate
Figure 3).
hypothalamic and pituitary response in terms of LH andprogesterone surge. Patients receiving physiological doses of
oestradiol and progesterone were shown to have a mid-cycleFSH increase resembling that occurring in the natural cycle.
The present data show how serum LH concentrations in
However, the LH surge was of lower amplitude, confirming
infertile patients undergoing IUI with spontaneous LH surge
the hypothesis that independent controls regulate FSH and LH
(>10 mIU/ml) and premature luteinization (serum
secretion (Taylor et al., 1995). It was also demonstrated that
progesterone concentrations >1 ng/ml) were not correlated
different formulations of gonadotrophins used for ovarian
with various characteristics of the treatment. These included
stimulation (HMG or recFSH) did not alter the nature of the
the ovarian stimulation protocol, oestradiol serum
LH surge or premature luteinization. Nor was the size of the
concentrations, dominant follicular size and total number of
dominant follicule in stimulated cycles any different to that
Article - Premature LH and progesterone rise in IUI - JS Cunha-Filho et al
occurring during natural cycles. Modulation of LH surge is
cannot be predicted utilizing the clinical parameters normally
probably very complex, and associated with different
employed (ultrasound and serum oestradiol assay). New
prospective studies are essential to confirm and extendavailable data. Nevertheless, patients with follicles >14 mm, or
The LH surge is naturally modulated by GnRH, and other
patients with many small follicles and high oestradiol, are at
hormones and peptides, e.g. GnSAF, which may induce it
risk of a spontaneous LH surge. In assisted reproduction
under special hormonal and metabolic environments
cycles, these criteria could be used to time the administration
(Loumaye, 1990; Fowler et al., 1993).
of GnRH antagonists until better predictive factors aredemonstrated. New studies will be welcome to isolate new
Recently, small follicles were shown to contain high
peptides offering better predictions of premature LH rise,
concentrations of GnSAF, which could prevent premature LH
investigating the role of inhibins and activins, and offering
surges during non-stimulated cycles (Fowler et al., 2001). The
prospective studies designed to elucidate follicular dynamics
present results are in agreement, and show how the premature
LH rise cannot be predicted. Similar conclusions haveemerged for progesterone increments, based only on clinical
JS Cunha-Filho was supported by a CAPES post-doctoral
The clinical impact of premature LH surges during IUI on
subsequent pregnancy rates was evaluated in patients givenhuman chorionic gonadotrophin (HCG) before the onset of
their LH surge (Fuh et al., 1997). However, the authors did not
Albano C, Smitz J, Camus M et al. 1997 Comparison of different
measure serum progesterone concentrations, so the impact of
doses of gonadotropin-releasing hormone antagonist Cetrorelix
premature luteinization in relation to the clinical outcome of
during controlled ovarian hyperstimulation. Fertility and Sterility
the patients could not be measured. Clinical outcomes were
67, 917–922.
not reported in this study, because several confounding biases
Borm G, Mannaerts B 2000 Treatment with the gonadotrophin-
can interfere with a specific clinical trial, and numbers of
releasing hormone antagonist ganirelix in women undergoing
ovarian stimulation with recombinant follicle stimulatinghormone is effective, safe and convenient: results of a controlled,randomized, multicentre trial. The European Orgalutran Study
Because the study design was retrospective and two different
Group. Human Reproduction 15, 1490–1498.
investigators measured the follicular diameters, the coefficient
Cahill DJ, Wardle PG, Harlow CR, Hull MGR. 1998 Onset of the
of variability (<15%) was extremely low, excluding the
preovulatory luteinizing hormone surge: diurnal timing and
possibility of significant bias. Nevertheless, a larger
critical follicular prerequisites. Fertility and Sterility 70, 56–59.
prospective trial is needed to clarify the exact nature of factors
Cahill DJ, Wardle PG, Harlow CR et al. 2000 Expected contribution
determining rising progesterone concentrations and premature
to serum estradiol from individual ovarian follicles in
unstimulated cycles. Human Reproduction 15, 1909–1912.
Christin-Maitre S, Olivennes F, Dubourdieu S et al. 2000 Effect of
GnRH antagonist during the LH surge in normal women and
The advent of the third generation of GnRH antagonist opens
during controlled ovarian hyperstimulation. Clinical
a new horizon in controlled ovarian stimulation. This
Endocrinology 52, 721–726.
compound can induce rapid and effective declines in LH
Costello MF, Hughes GJ, Garret DK et al. 1998 A spontaneous
secretion, even as the initial LH rise is in progress (Christin-
luteinizing hormone surge is beneficial in women with
Maitre et al., 2000). However, a premature LH surge, or the
unexplained infertility undergoing controlled ovarian
selection of patients at risk, cannot be predicted from their
hyperstimulation without in vitro fertilization. International
clinical or laboratory characteristics, due to the variability and
Journal of Fertility 43, 28–33.
complexity of associated variables. The scheduled
Couzinet B, Schaison G 1993 The control of gonadotrophin secretion
by ovarian steroids. Human Reproduction 8, 97–101.
administration of GnRH antagonists in patients developing a
De Boever J, Kohen F, Vandekerckhove D 1983 Solid-phase
premature LH surge offers an interesting alternative, but
chemiluminescence immunoassay for plasma estradiol-17 beta
requires a large randomized trial to evaluate reproductive
during gonadotropin therapy compared with two
radioimmunoassays. Clinical Chemistry 29, 2068–2072.
Eibschitz I, Belaisch-Allart JC, Frydman R 1986 In vitro fertilization
Patients with >2 follicles and higher oestradiol secretion
management and results in stimulated cycles with spontaneous
should be managed with special care, to prevent a premature
luteinizing hormone discharge. Fertility and Sterility 45,
LH rise, compared with those having only one follicle. In
Eissa MK, Obhrai MS, Docker MF et al. 1986 Follicular growth and
addition, spontaneous cycles demonstrate an important
endocrine profiles and induced conception cycles. Fertility and
hormonal profile, with premature LH surges occurring when
Sterility 45, 191–195.
the dominant follicle reaches 17 mm (15.5–18). This differs
Fanchin R, Righini C, Olivennes F et al. 1996 Premature
from classically described values of 20 mm (range 18–26
progesterone elevation does not alter oocyte quality in in vitro
mm). This discrepancy can be explained by the different
fertilization. Fertility and Sterility 65, 1178–1183.
technologies now employed for follicular measurement
Fowler PA, Templeton A, Messinis IE 1993 The ovarian modulation
(Gougeon and Lefèvre, 1983; Loumaye, 1990).
of gonadotrophin releasing hormone-induced luteinizing hormone secretion on women. Human Reproduction 8, 112–116.
Fowler PA, Sorsa T, Harris WJ et al. 2001 Relationship between
In conclusion, the study and prediction of premature LH and
follicle size and gonadotrophin surge attenuating factor (GnSAF)
progesterone surges are important in assisted reproduction.
bioactivity during spontaneous cycles in women. Human
The data presented in this study show that the initial LH rise
Reproduction 16, 1353–1358.
Article - Premature LH and progesterone rise in IUI - JS Cunha-Filho et al
Freimanis MG, Jones AF 1992 Transvaginal ultrasonography. Radiolic Clinics of North America 30, 955–976.
Fuh KW, Wang X, Tai A et al. 1997 Intrauterine insemination: effect
of the temporal relationship between the luteinizing hormone surge, human chorionic gonadotrophin administration and insemination on pregnancy rates. Human Reproduction 12, 2162–2166.
Gougeon A, Lefèvre B 1983 Evolution of the diameters of the largest
healthy and atretic follicles during the human menstrual cycle. Journal of Reproductive Fertility 69, 497–502.
Hershlag A, Zinger M, Lesser M et al. 2000 Is chemiluminescent
immunoassay an appropriate substitution for radioimmunoassay in monitoring estradiol levels? Fertility and Sterility, 73 1174–1178.
Kagawa T, Yamano S, Nishida S et al. 1992 Relationship among
serum levels of luteinizing hormone, estradiol, and progesterone during follicle stimulation and results of in vitro fertilization and embryo transfer (IVF–ET). Journal of Assisted Reproduction and Genetics, 9 106–112.
Kreiner D, Droesch K, Itskovitz J et al. 1988 Spontaneous
luteinizing hormone (LH) surges are associated with more rapidly increasing estradiol and follicle stimulating hormone in in vitro fertilization and embryo transfer. Journal of In Vitro Fertilization and Embryo Transfer 5, 265–267.
Loumaye E 1990 The control of endogenous secretion of LH by
gonadotrophin-releasing hormone agonists during ovarian hyperstimulation for in vitro fertilization and embryo transfer. Human Reproduction 5, 357–376.
McCartney CR, Gingrich MB, Hu Y et al. 2002 Hypothalamic
regulation of cyclic ovulation: evidence that the increase in gonadotropin-releasing hormone pulse frequency during the follicular phase reflects the gradual loss of the restraining effects of progesterone. Journal of Clinical Endocrinology and Metabolism 87, 2194–2200.
Macnamee MC, Edwards RG, Howles CM 1988 The influence of
stimulation regimes and luteal phase support on the outcome of IVF. Human Reproduction 3 (suppl. 2), 43–52.
Olivennes F, Alvarez S, Bouchard P et al. 1998 The use of a GnRH
antagonist (Cetrorelix) in a single dose protocol in IVF–embryo transfer: a dose finding study of 3 versus 2 mg. Human Reproduction 13, 2411–2414.
Taylor AE, Whitney H, Hall JE et al. 1995 Midcycle levels of sex
steroids are sufficient to recreate the follicle-stimulating hormone but not the luteinizing hormone midcycle surge: evidence for the contribution of other ovarian factors to the surge in normal women. Journal of Clinical Endocrinology and Metabolism 80, 1541–1547.
Testart J, Frydman R. 1982 Minimum time lapse between luteinizing
hormone surge or human chorionic gonadotropin administration and follicular rupture. Fertility and Sterility 37, 50–53.
Testart J, Frydman R, Roger M 1982 Seasonal influence of diurnal
rhythms in the onset of the plasma luteinizing hormone surge in women. Journal of Clinical Endocrinology and Metabolism 55, 374–377. Received 20 February 2003; refereed 3 April 2003; accepted18 April 2003.
OperaOnline.us Worldwide reviews for a worldwide audience LA Opera’s ‘Otello’ – A Poignant Production with Lush Choral Lyricism Photo: Robert Millard GIUSEPPE VERDI OTELLO LOS ANGELES OPERA FEBRUARY 16, 2008 By: Carol Jean Delmar OperaOnline.us The buzz going around is that there’s a bug loose backstage in LA Opera’s Dorothy Chandler Pavilion. Many of the singers
HÉMA-VIGIE…always on the lookout! A Monthly Newsletter Summarizing Important Advances in Transfusion Volume 3, Number 1 West Nile virus – infected birds: an early tral role in the peripheral circulation problems commonly warning sign of upcoming human infec- encountered in sickle-cell disease patients. Reiter, C. D., et al. (2002). Cell-free hemoglobin limits nit
 RBMOnline - Vol 7. No 2. 194–199 Reproductive BioMedicine Online; www.rbmonline.com/Article/894 on web 16 June 2003
Premature LH and progesterone rise inintrauterine insemination cycles: analysis ofrelated factors
João Sabino Cunha-Filho obtained his MD degree (1993) and the speciality degree inObstetrics and Gynecology (1997) at the Faculty of Medicine (Hospital de Clínicas de PortoAlegre, Universidade Federal do Rio Grande do Sul) in Brazil. The PhD degree was grantedto him at the same University in 2000. He continued with post-doctoral studies at Clamart,France (2001). At present he is Professor in Obstetrics and Gynaecology at the Faculty ofMedicine–Hospital de Clínicas de Porto Alegre in Brazil and has authored more than 150publications in national and international journals and books. His current research interestsinclude assisted reproduction, endometriosis and ovarian stimulation.
RBMOnline - Vol 7. No 2. 194–199 Reproductive BioMedicine Online; www.rbmonline.com/Article/894 on web 16 June 2003
Premature LH and progesterone rise inintrauterine insemination cycles: analysis ofrelated factors
João Sabino Cunha-Filho obtained his MD degree (1993) and the speciality degree inObstetrics and Gynecology (1997) at the Faculty of Medicine (Hospital de Clínicas de PortoAlegre, Universidade Federal do Rio Grande do Sul) in Brazil. The PhD degree was grantedto him at the same University in 2000. He continued with post-doctoral studies at Clamart,France (2001). At present he is Professor in Obstetrics and Gynaecology at the Faculty ofMedicine–Hospital de Clínicas de Porto Alegre in Brazil and has authored more than 150publications in national and international journals and books. His current research interestsinclude assisted reproduction, endometriosis and ovarian stimulation.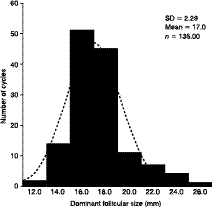
 Article - Premature LH and progesterone rise in IUI - JS Cunha-Filho et al
Figure 1. Distribution of surges of dominant follicles (mm)
Article - Premature LH and progesterone rise in IUI - JS Cunha-Filho et al
Figure 1. Distribution of surges of dominant follicles (mm)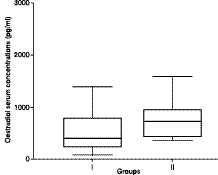
 Article - Premature LH and progesterone rise in IUI - JS Cunha-Filho et al
Table 2. Multiple regression analysis (dependent variable:
Article - Premature LH and progesterone rise in IUI - JS Cunha-Filho et al
Table 2. Multiple regression analysis (dependent variable: