STRAIN ENCODED (SENC) IMAGING FOR DETECTION OF REGIONAL DYSFUNCTION IN PATIENTS WITH MYOCARDIAL INFARCTION AT 3T Li Pan, MS,1 Ahmed S. Fahmy, MS,2 Amy Spooner, MD,1 Robert G. Weiss, MD,1 Matthias Stuber, PhD,1 Nael F. Osman, PhD.1 1Johns Hopkins School of Medicine, Bal- timore, MD, USA, 2Johns Hopkins University, Baltimore, MD, USA.
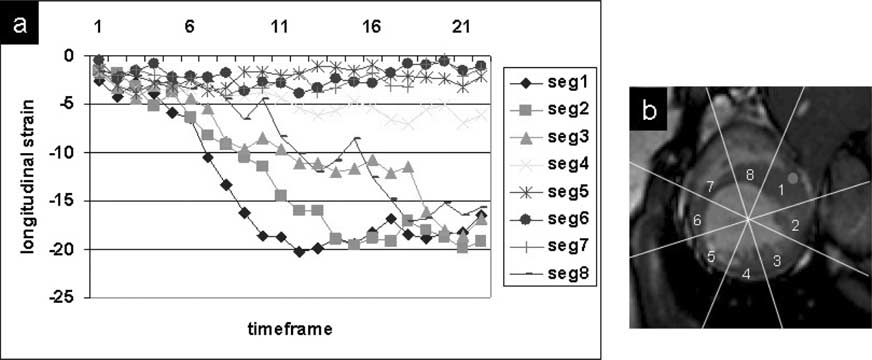
(a) Longitudinal strain measurments by segments in short-axis view
Introduction: SENC imaging (1) is a technique that can directly
from one patient. (b) The eight segments defined clockwise in the short-axis
image and quantify regional myocardial function. It has been
view, shown on the SSFP image, with the isertion point of the right ventricle
demonstrated that SENC imaging on a 3T system provides sim-
(green spot) as mid-point of the first segment.
ilar strain measurements in normal subjects as those acquired at1.5T and offers improvements in SNR (2). In this study, SENC
travenous contrast, 0.2 mmol.kg−1Gd-DTPA, was injected. Fif-
imaging sequences, implemented on 3T MR scanner, have been
teen minutes later, an inversion-recovery (IR)-prepared, fast field
used to study patients with a history of myocardial infarction.
echo (FFE) pulse sequence with inversion time (TI) = 300 ms
The dysfunctional regions detected by SENC acquisition have
was performed to obtain a delayed enhancement image for the
been compared with those identified by delayed enhancement
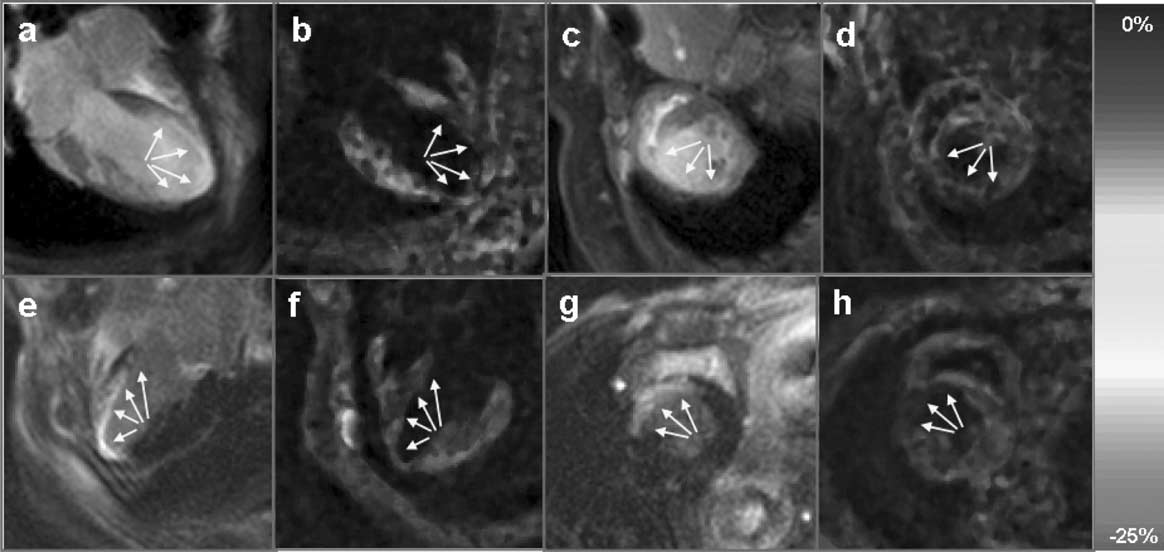
Results: Fig. 1 shows representative results of SENC imaging
Purpose: To demonstrate that SENC imaging can provide
from two patients, each row represents a different patient. In both
reliable evaluation of regional dysfunction of the heart in patients
four-chamber and short-axis views, the comparison of the areas
with a history of myocardial infarction on a 3T MR scanner.
of myocardial dysfunction detected by SENC imaging (Fig. 1
Methods: Following informed consent, the studies were per-
b,d,f,h) to the nonviable myocardium defined by hyperenhanced
formed on a clinical 3T MR whole body scanner (Achieva,
tissue in the delayed enhancement images (Fig. 1 a,c,e,g) shows
Philips Medical System, Best, The Netherlands). Five patients
high agreement. Fig. 2a shows representative results of longitu-
(four males, one female) with a history of myocardial infarction
dinal strain measurements of eight segments, defined in Fig. 2b,
were imaged in both short-axis and four-chamber views. SENC
on short-axis SENC images. Segments 5,6,7 are infarcted re-
images were acquired in one breath-hold with low-tuning and
gions, which show no contraction, segments 3,4,8 are adjacent
high-tuning interleaved in one acquisition. A total of 19 to 23
regions, which show reduced contraction, and segments 1,2 are
time frames were acquired to cover systole. The tuning spa-
remote non-infarcted regions, which show normal contraction.
tial frequencies were set as 0.3 mm−1 and 0.4 mm−1 for low-
Conclusions: Despite the inherent challenges for cardiac
tuning and high-tuning respectively. The imaging parameters
imaging at 3T, the SENC imaging has been demonstrated to
were: slice thickness = 10 mm, FOV = 350 mm, matrix size =
be able to detect the regional dysfunction of the heart in pa-
176 × 176, spiral interleaves = 12, spiral acquisition window =
tients with a history of myocardial infarction. The identified
12 ms, max ramped flip angle = 40. After SENC acquisition, in-
dysfunctional regions show high agreement with those defined
Representative results from two patients (patient 1: first row, patient 2: second row) in both four-chamber (first two columns) and short-axis view (last two
columns). The SENC functional images (b,d,f,h) showing regional dysfunction (arrows) were compared with the delayed-enhancement images (a,c,e,g) showinghyperenhanced nonviable infarcted myocardium (arrows).
by delayed enhancement imaging. SENC imaging on 3T MR
system allows determination of regional myocardial function,
with high spatial resolution, in infarcted, adjacent, and remotehuman myocardium. Acknowledgements: This research was supported by grant
RO1 HL072704 and by support from the Donald W. Reynolds
REFERENCES
1. Osman NF, et al. Magn Reson Med 2001;46:324–334. 2. Pan L, et al. SCMR 2005, #397. BASELINE PATIENT CHARACTERISTICS FOR THE MRI SUBSTUDYTO ONTARGET Brett R. Cowan, BE MbChB, Alistair A. Young, BE ME PhD, on behalf of the ONTARGET MRI Substudy Investigators. University of Auckland, Auckland, New Zealand.
informed consent, uncontrolled hypertension on treatment, hearttransplant or stroke due to subarachnoid haemorrhage (1). Sub-
Introduction: ONTARGET (ONgoing Telmisartan Alone and
study exclusion criteria included MRI contraindications. Writ-
in combination with Ramipril Global Endpoint Trial) is a world-
ten informed consent was obtained from all subjects and regula-
wide, multi-center, controlled clinical trial investigating the ef-
tory authorities of local participating institutions in all countries
fects of ramipril and the angiotensin II receptor blocker telmisar-
approved the study protocol. The MR imaging protocol was
tan, alone and in combination, in high-risk subjects with vascular
standardized across 8 imaging centers. Subjects were imaged
disease (1). Major cardiovascular events are being assessed to
for the baseline examination during week 3 (plus or minus 1
test for reduction in composite outcome (1). In order to investi-
week) of the run in phase of the trial (ie an average of one week
gate mechanistic pathways in these therapies, a MRI substudy
prior to randomization and commencement on study medica-
will determine whether the effects of these agents involve direct
tion). Steady state free precession anatomical cine images were
actions on LV mass and volume, as determined by MRI.
acquired in six equally spaced short axis locations from apex
Purpose: i) To report the baseline characteristics for subjects
to base and three long axis slices orthogonal to the short axis
enrolled in the MRI substudy to ONTARGET. ii) To examine
and orientated at 60 degree increments about the central axis
differences in LV mass and volumes between Asian and non-
of the LV. Typical imaging parameters were TR/TE/flip/FOV =
30 ms/1.6 ms/60◦/360 mm, slice thickness 6 mm, image matrix
Methods: The Cardiac MRI substudy to ONTARGET com-
256 × 208, 25 frames reconstructed, 8–15 sec breath-hold du-
prised 28 recruiting centers in 6 countries (Australia, New
ration. All MRI studies were digitally recorded onto CD-ROM
Zealand, Germany, Canada, Thailand and Hong Kong); 330
and sent to the core lab for analysis. LV mass and volumes were
patients were enrolled between October 2002 and July 2003.
determined using guide point modelling (2).
Patients were included with myocardial infarction (MI), coro-
Results: Table 1 shows basic patient characteristics. LV mass
nary or peripheral arterial disease (CAD, PAD), cerebrovascular
and volumes are shown in Table 2. LV mass, EDV and ESV
disease (CVD) or high-risk diabetes mellitus (DM) with end-
were smaller in Asians vs non-Asians (p < 0.001 for each).
organ damage (1). Patients were excluded with symptomatic
However, on normalization with the allometric index Height2.7,
congestive heart failure, significant valvular disease, complex
the differences between ethnic groups wereas eliminated (p =
congenital heart disease, syncopal episodes of unknown aetiol-
ogy, planned cardiac surgery or PTCA within three months of
Conclusion: Baseline characteristics for the MRI substudy
to ONTARGET cover a wide range of patient diagnoses. LV
mass and volume measurements from these patients provide
useful data on population variation in cardiovascular disease.
The allometric index Height2.7 normalized LV mass and volumes
between Asian and non-Asian cohorts. REFERENCES
1. Teo KK, et al. Am Heart J 2004;148:52–61.
2. Young AA, et al. Radiology 2000; 216:597–602.
ETSÄMÄEN PELIVIHJEET L OUNASRAVIT PERJANTAINA 24.4.2009 Lähtö 1 A) 2,1 / B) 9,4,12,3,5,10,7,6 / C) 8,11 2 RAINBOW YASMIN osoitti hyviä kyytejä jo viime vuonna. Tamma kokee nyt melkoisen kuskinvahvistuksen, joten sopivassa seurassa sen kuuluu ravia mennessään pärjätä. 1 KING CHAPELWAY on tähän porukkaan kyvykäs menijä. Helmikuussa sen oli määrä startata Vermossa, m
INSTRUCTIONS FOR USE TO REPLACE BATTERIES TO REMOVE TRAY/COVER TO SWITCH ON PRESS TO COVERT WEIGHT UNITS TO ADD & WEIGH AUTO SWITCH OFF MANUAL SWITCH OFF Press the button on the left side of the scale and 1) Place tray on scale before switching on. Press g button to convert between To weigh several different ingredients inTo maximise battery life press and releas
 STRAIN ENCODED (SENC) IMAGING FOR
STRAIN ENCODED (SENC) IMAGING FOR