Salpingectomy for hydrosalpinx prior to in vitro fertilization
Salpingectomy for hydrosalpinx prior to in vitrofertilization
Practice Committee of the American Society for Reproductive Medicine in collaboration with TheSociety of Reproductive Surgeons
The American Society for Reproductive Medicine, Birmingham, Alabama
Salpingectomy for hydrosalpinges before in vitro fertilization increases the success rate. (Fertil SterilÒ2008;90:S66–8. Ó2008 by American Society for Reproductive Medicine.)
In vitro fertilization (IVF) generally is accepted as the treat-
dence interval [CI], 41.4–62.2) The effect was observed
ment of choice for women with distal tubal occlusive disease
in both fresh and frozen embryo transfer cycles. The likeli-
who wish to conceive; the role of tubal reconstructive surgery
hood of miscarriage also was 2.3-fold (95% CI, 1.6–3.5)
is quite limited. Whereas surgery still may be considered for
higher among women with hydrosalpinges. The likelihood
selected young women (<age 35 years) with mild tubal dis-
of ectopic pregnancy could not be evaluated precisely even
ease and no other coexisting infertility factors and for those
in this data set, suggesting a small, if any, effect on ectopic
who reject or have no practical access to IVF, the outcomes
rates. A second meta-analysis included nine published studies
achieved with surgery otherwise are almost uniformly poor
and five abstracts involving 5592 women, including many of
Evidence indicates that the presence of hydrosalpinges
the same studies used in the first meta-analysis Delivery
adversely affects results achieved with IVF, decreasing live
rates per cycle start were 13.4% in 1418 cycles with hydrosal-
birth rates by approximately 50% Whether these ad-
pinx and 23.4% in 6735 cycles without hydrosalpinx (OR
verse effects are common to all hydrosalpinges or may be
limited to those that are larger and thus visible with transva-ginal ultrasonography remains uncertain Treatment ofhydrosalpinges by salpingectomy or by proximal tubal occlu-
sion improves results achieved with subsequent IVF. The pur-
The effect of interrupting proximal tubal patency or salpin-
pose of this document is to review these data and the
gectomy on the outcomes achieved with subsequent IVF
pathophysiologic mechanisms that may explain the observa-
has been assessed in three randomized controlled trials
(RCTs). One was a pilot study that included 60 patientswith hydrosalpinges or proximal tubal disease related to sal-pingitis isthmica nodosa who underwent laparoscopy; 30
women were treated by salpingectomy, and, in the remaining
A number of mechanisms have been proposed to explain the
30, the tubes were left intact. Unfortunately, the results for
adverse effects of hydrosalpinges on the live birth rate
patients with proximal occlusion do not address the primary
achieved with IVF. These include a direct embryotoxic effect
question and reduce the power of the already small study. The
a decrease in endometrial receptivity, and the possibility
pregnancy rates per cycle were 23.7% (14 of 59) after salpin-
that tubal fluid may mechanically flush the embryo from the
gectomy and 16.3% (8 of 49) without salpingectomy; the on-
going pregnancy rates per embryo transfer were 34.2% (13 of38) after salpingectomy and 18.7% (6 of 32) without salpin-
Several early reports indicated that the presence of unilateral
In a trial involving 204 patients with hydrosalpinges, the
or bilateral hydrosalpinges adversely affects implantation and
delivery rates were 28.6% in the 116 patients randomized
pregnancy rates achieved with IVF. Outcomes have been sum-
to salpingectomy before IVF and 16.3% in the 88 who did
marized in two meta-analyses. The first included over 6700
not receive preliminary surgical treatment (P¼.045) . In
treatment cycles from 11 studies, four of which were pub-
a subgroup analysis limited to patients having hydrosalpinges
lished only as abstracts. The pregnancy rate observed among
that were visible with ultrasonography, the corresponding
women with hydrosalpinges (165 pregnancies/1004 cycles;
delivery rates with and without preliminary salpingectomy
16.4%) was 49% lower than that observed in women with
were 40.0% and 17.5%, respectively (P¼.038).
tubal factor infertility without hydrosalpinges (1478 pregnan-
A third RCT involving 115 patients compared the results
cies/4736 cycles; 31.2%) (odds ratio [OR] 50.7; 95% confi-
observed after laparoscopic salpingectomy or proximal tubalocclusion with those in control women who received no sur-
gical treatment The ongoing pregnancy rates after the
Revised August 2008. No reprints will be available.
first embryo transfer were 37.8% with 45 transfers after
Fertility and Sterilityâ Vol. 90, Suppl 3, November 2008
Copyright ª2008 American Society for Reproductive Medicine, Published by Elsevier Inc.
salpingectomy, 48.9% with 47 transfers after proximal tubal
residing within the uterine cavity may exert a contraceptive
occlusion, and 7.1% after 14 transfers in control patients.
effect similar to that of an intrauterine device. A small
Both procedures produced statistically significantly better
observational study found that eight of 17 patients (47%)
results than no surgical intervention, and the outcomes
with hydrosalpinges who were treated with doxycycline for
achieved with the two surgical treatments were not materially
1 week before and after oocyte retrieval achieved a live birth,
different (P¼.20) Whether proximal tubal occlusion may
compared with 11 of 25 (44%) patients with proximal tubal
induce expansion of hydrosalpinges that may require later
occlusion or pelvic adhesions and 12 of /22 (55%) women
and more extensive surgical treatment is unknown.
with endometriosis or unexplained infertility who receivedno such treatment . At least in theory, neosalpingostomy
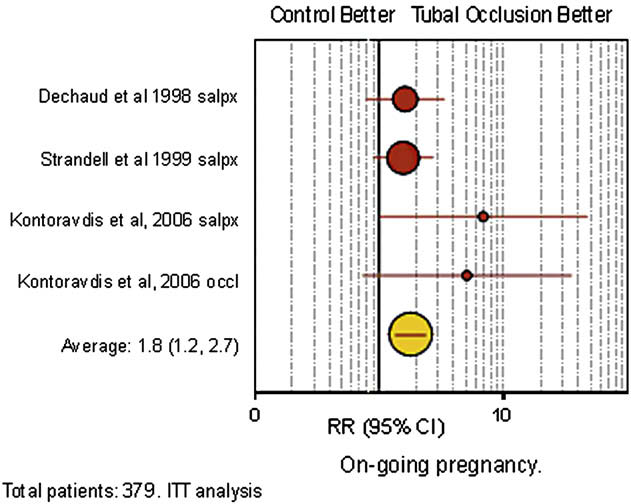
Based on results from the three trials, the ongoing
may effectively negate the adverse effect of hydrosalpinges
pregnancy rate after laparoscopic salpingectomy or tubal
on IVF outcomes while also permitting the possibility of
occlusion (34%) is twofold higher than in controls (17%)
natural conception, but no clinical studies have examined
). The 17% rate difference implies that for every six
(95% CI, 3–9) women with hydrosalpinges, one more ongo-ing pregnancy will be achieved if salpingectomy or tubalocclusion is performed before IVF.
1. The live birth rate achieved with IVF among women
with hydrosalpinges is approximately one half thatobserved in women without hydrosalpinges.
Options other than salpingectomy or proximal tubal occlu-
2. In women with hydrosalpinges, preliminary laparo-
sion have not been adequately evaluated in RCTs. Transvagi-
scopic salpingectomy or proximal tubal occlusion
nal aspiration of the hydrosalpinges during oocyte retrieval
improves subsequent pregnancy and live birth rates
was unsuccessful in one study and possibly helpful in an-
achieved with IVF. For every six women with hydrosal-
other . Another RCT observed that clinical pregnancy
pinges, one more ongoing pregnancy will be achieved if
rates were 31.3% (10 of 32) after aspiration and 17.6% (6
salpingectomy or tubal occlusion is performed before
of 34) without (RR ¼ 1.8; 95% CI, 0.8–4.3; P¼.2)
Two reports have described three women with hydrosal-
3. Data are insufficient to permit recommendations
pinges who conceived via IVF after hysteroscopic placement
regarding the effectiveness of alternative treatments
of the Essureâ (Conceptus, Mountain View, CA) microinsert
such as laparoscopic neosalpingostomy, transvaginal
device A small case series found that bilateral place-
aspiration of hydrosalpingeal fluid, hysteroscopic tubal
ment of the Essureâ device could be accomplished only in
two of five patients with hydrosalpinges; neither of the twowomen who subsequently underwent IVF conceived
Acknowledgments: This report was developed under the direction of the Prac-
There is also the possibility that the portion of the device
tice Committee of the American Society for Reproductive Medicine and theSociety of Reproductive Surgeons as a service to its members and other prac-ticing clinicians. Although this document reflects appropriate management ofa problem encountered in the practice of reproductive medicine, it is not in-
tended to be the only approved standard of practice or to dictate an exclusivecourse of treatment. Other plans of management may be appropriate, taking
Effect of treating hydrosalpinges before in vitro
into account the needs of the individual patient, available resources, and insti-
tutional or clinical practice limitations. This report was approved by the Prac-tice Committee of the American Society for Reproductive Medicine and theBoard of Directors of the American Society for Reproductive Medicine.
1. Practice Committee of the American Society for Reproductive Medicine.
The role of tubal reconstructive surgery in the era of assisted reproductivetechnologies. Fertil Steril 2006;86(Suppl):S31–4.
2. Zeyneloglu HB, Arici A, Olive DL. Adverse effects of hydrosalpinx on
pregnancy rates after in vitro fertilization–embryo transfer. Fertil Steril1998;70:492–9.
3. Camus E, Poncelet C, Goffinet F, Wainer B, Merlet F, Nisand I, et al.
Pregnancy rates after in-vitro fertilization in cases of tubal infertilitywith and without hydrosalpinx: a meta analysis of published comparativestudies. Hum Reprod 1999;14:1243–9.
4. de Wit W, Gowrising CJ, Juik DJ, et al. Only hydrosalpinges visible on
ultrasound are associated with reduced implantation and pregnancy ratesafter in-vitro fertilization. Hum Reprod 1998;13:1606–701.
5. Mukherjee T, Copperman AB, McCaffrey C, Cook CA, Bustillo M,
Obasaju MF. Hydrosalpinx fluid has embryotoxic effects on murine em-brogenesis: a case for prophylactic salpingectomy. Fertil Steril 1996;66:
ASRM Practice Committee. Salpingectomy for hydrosalpinx. Fertil Steril 2008.
6. Dechaud H, Daures JP, Arnal F, Humeau C, Hedon B. Does previous sal-
and implantation rates after in-vitro fertilization cycles. Hum Reprod
pingectomy improve implantation and pregnancy rates in patients with
severe tubal factor infertility who are undergoing in vitro fertilization?
11. Hammadieh N, Coomarasamy A, Ola B, Papaioannou S, Afnan M,
A pilot prospective randomized study. Fertil Steril 1998;69:1020–5.
Sharif K. Ultrasound-guided hydrosalpinx aspiration during oocyte col-
lection improves pregnancy outcome in IVF: a randomized controlled
Hamberger L. Hydrosalpinx and IVF outcome: a prospective, randomized
multicentre trial in Scandinavia on salpingectomy prior to IVF. Hum
12. Rosenfield RB, Stones RE, Coates A, Matteri RK, Hesla JS. Proximal oc-
clusion of hydrosalpinx by hysteroscopic placement of microinsert be-
8. Kontoravdis A, Makrakis E, Pantos K, Botsis D, Deligeoroglou E,
fore in vitro fertilization–embryo transfer. Fertil Steril 2005;83:1547–50.
Creatsas G. Proximal tubal occlusion and salpingectomy result in similar
13. Kerin JF, Cattanach S. Successful pregnancy outcome with the use of
improvement in in vitro fertilization outcome in patients with hydrosal-
in vitro fertilization after Essure hysteroscopic sterilization. Fertil Steril
pinx. Fertil Steril 2006;86:1642–9.
9. Sowter MC, Akande VA, Williams JA, Hull MG. Is the outcome of in-vi-
14. Hitkari JA, Singh SS, Shapiro HM, Leyland N. Essure treatment of
tro fertilization and embryo transfer treatment improved by spontaneous
hydrosalpinges. Fertil Steril 2007;88:1663–6.
or surgical drainage of a hydrosalpinx? Hum Reprod 1997;12:2147–50.
15. Hurst BS, Tucker KE, Awoniyi CA, Schlaff WD. Hydrosalpinx treated
10. Van Voorhis BJ, Sparks AE, Syrod CH, Stoval DW. Ultrasound-guided
with extended doxycycline does not compromise the success of in vitro
aspiration of hydrosalpinges is associated with improved pregnancy
fertilization. Fertil Steril 2001;75:1017–9.
PRODUCT SAFETY DATA SHEET INSECTICIDE 1. Identification of the substance/preparation and company PRODUCT NAME: Insecticide PRODUCT USE: For the control of crawling and flying insects. SUPPLIER: Eastby Services Limited t/a Alltec Network Butts Farm, Fowlmere, Nr Royston, Herts EMERGENCY TEL No. 01763-208222 01763-208906 2. Composition/inf
PAGE 54 / MAY 25, 2008 S C R I P T D O C T O R : M E D I C I N E I N T H E M E D I A Dateline Nigeria (Part 3): Creating Solutions When Despite Public Service Announcements, Ads, & Documentaries, Many Women Were Still Not Seeking Life-Saving Treatment that was created aftera well-meaning health Andrew Holtz, MPH, is a “S ànnu.” former CNN Medical Corresponden
 salpingectomy, 48.9% with 47 transfers after proximal tubal
residing within the uterine cavity may exert a contraceptive
occlusion, and 7.1% after 14 transfers in control patients.
salpingectomy, 48.9% with 47 transfers after proximal tubal
residing within the uterine cavity may exert a contraceptive
occlusion, and 7.1% after 14 transfers in control patients.