P a t h o p h y s i o l o g y / C o m p l i c a t i o n s O R I G I N A L Influence of Caffeine on Heart Rate Variability in Patients With Long- Standing Type 1 Diabetes RISTAN RICHARDSON, MRCP JACQUELINE RYDER DRIAN ROZKOVEC, FRCP CANDY MECKES, BSC ETER THOMAS, PHD DAVID KERR, FRCP
(Ͼ5 years) type 1 diabetes and 10 controlsubjects with similar sex and age distribu-tion and without evidence of cardiovascu-lar disease (Table 1) participated in adouble-blind, randomized crossover, pla-
OBJECTIVE — The effect of caffeine on cardiovascular health remains controversial. Patients
cebo-controlled study of the effects of caf-
with long-standing type 1 diabetes are at risk of autonomic failure and sudden cardiac death. We
investigated the effects of caffeine on autonomic dysfunction (as assessed by heart rate variability
[HRV]) in this high-risk group and in a control population. RESEARCH DESIGN AND METHODS — Using a randomized blinded, placebo-
controlled, crossover design trial, we examined 2 weeks of caffeine consumption (250 mg twice
daily) on HRV in 20 type 1 diabetic patients and 10 matched healthy volunteers.
screened by 12-lead electrocardiogram(ECG), echocardiography, and treadmill
RESULTS — Baseline HRV was blunted in the diabetic patients (P Ͻ 0.0005 vs. control
exercise testing. Those with atrial fibrilla-
subjects) and markedly increased by caffeine in both groups (ϩ103% in the group with diabetes
[P ϭ 0.009] and ϩ38% in control subjects [P ϭ 0.002]). The caffeine-associated increase in HRV
of left ventricular systolic impairment (left
was not statistically different between the control and the type 1 diabetes groups (P ϭ 0.16). CONCLUSIONS
— Modest amounts of caffeine improved autonomic function in diabetic
patients and healthy volunteers. For individuals with abnormal HRV, regular caffeine use may
have the potential to reduce the risk of cardiovascular events.
dicted heart rate during or after exerciseusing the Bruce protocol) were excluded. Diabetes Care 27:1127–1131, 2004
No patients had renal failure. All controlsubjects had normal beats for at least 99%of total QRS complexes on 24-h ambula-
Reducedheartratevariability(HRV), neuroglycopeniadevelops(5).Ingestion toryECGmonitoring.
subjects is associated with detectable car-
diovascular changes, including a transient
disease and sudden death in both diabetic
increase in blood pressure, although these
and nondiabetic populations (1,2). In pa-
lent to average caffeine intake in the U.K.)
ever, the effects of ingestion of caffeine on
effect of caffeine on HRV in patients with
in type 1 diabetic patients at risk of hypo-
long-standing type 1 diabetes and healthy
glycemia (4). The intensity of early warn-
RESEARCH DESIGN AND
interstitial glucose levels using the contin-
METHODS — All subjects provided
viduals to take appropriate action before
system (CGMS) (7). The patients andcontrol subjects were crossed over to the
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
alternate treatment arm, and the final set
From the 1Bournemouth Diabetes & Endocrine Centre, Bournemouth, U.K.; the 2Department of Cardiology,
Royal Bournemouth Hospital, Bournemouth, U.K.; and 3Dorset Research and Development Unit &
Bournemouth University, Bournemouth, U.K.
Address correspondence and reprint requests to Dr. Tristan Richardson, Bournemouth Diabetes & En-
docrine Centre, Royal Bournemouth Hospital, Castle Lane East, Bournemouth, BH7 7DW, U.K. E-mail:
[email protected].
Received for publication 20 November 2003 and accepted in revised form 10 February 2004. Abbreviations: CGMS, continuous glucose monitoring system; ECG, electrocardiogram; HF, high fre-
quency; HRV, heart rate variability; LF, low frequency; sNN , sum of mean RR intervals
2004 by the American Diabetes Association.
DIABETES CARE, VOLUME 27, NUMBER 5, MAY 2004
Caffeine and heart rate variability Table 1—Details of participants
type 1 diabetic patients was 70 Ϯ 72counts per hour and was significantly
trol subjects (213 Ϯ 86 counts per hour,
[95% CI 78 –205], P ϭ 0.0005 using in-
dependent samples t test) (Fig. 1).
([95% CI 34 –173], mean increase [ϮSD]
CI 10 – 63], P ϭ 0.009) and in healthy
83], P ϭ 0.002) when compared with pla-
Data are n, means Ϯ SD, or % (n). *ACE inhibitor or angiotensin-receptor blocker.
was not statistically different between thecontrol and the type 1 diabetic groups(mean percentage difference 70% [95%
relayed through a Pathfinder 700 arrhyth-
CI Ϫ27 to 168], P ϭ 0.16; mean abso-
mia analyzer. After initial arrhythmia as-
Smirnov Z statistics had P values of
Ͼ0.05). Comparison of changes between (Fig. 2).
ple with diabetes and healthy control sub-
jects were made using the paired t test,
made using the independent samples t
domized to placebo or caffeine first. The
subjects randomized to caffeine first were
movement artifacts. A fast Fourier trans-
considered to be “caffeine tolerant”—they
each hour over the 48 h of ECG recording,
feine-replete diet to ongoing caffeine sup-
plementation. The “caffeine naı¨ve”
rected for filtering and sampling effects.
placebo phases. All tests were two tailed
and used a 5% critical P value.
introduction to caffeine on the active arm.
power (0.04 – 0.15 Hz) reflects modula-
RESULTS — Clinical and laboratory
characteristics of the diabetic and control
tone by baroreflex activity, and the high
for each subject. There was no statistically
frequency (HF) power (0.15– 0.4 Hz) re-
significant difference (P ϭ 0. 80) in the
flects modulation of vagal tone (parasym-
ilar to our clinic type 1 diabetic popula-
tolerant and caffeine-naı¨ve groups, dem-
onstrating that the influence of caffeine on
HRV did not attenuate with sustained use.
tachycardia, aberrant beats, or ventricular
version 11. For each individual at the end
CONCLUSIONS — In this study, in-
tistics were then used for the data analy-
teers and diabetic patients. There was no
DIABETES CARE, VOLUME 27, NUMBER 5, MAY 2004
Richardson and Associates
ties of HRV may precede clinical expres-sion of autonomic failure (20). Someinvestigators have described an associa-tion between autonomic dysfunction andabnormal cardiac repolarization, mani-fested by a prolonged QT interval(21,22). These abnormalities may predictsubsequent fatal ventricular dysrhyth-mias and sudden death. Factors exacer-b a t i n g Q T p r o l o n g a t i o n i n c l u d ehypokalemia, which may be provoked bylow prevailing glucose (23) and by hypo-glycemia per se (24). We did not find aconsistent relationship between fluctua-tions in interstitial glucose levels as as-sessed by the CGMS and HRV.
provement in HRV, values do still fallshort of the normal range. However, theincrease is still important. With oldertechnology, subtle differences in HRV
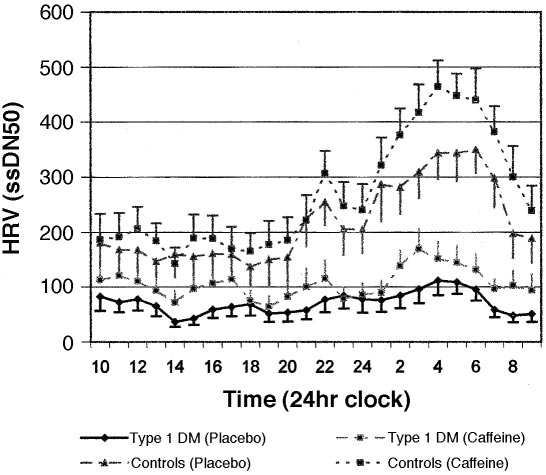
Figure 1—Diurnal variation of HRV (as measured by total sNN
were missed, and only cases with severely
over 48 h) and the influence of caffeine in type 1 diabetic and control groups.
impaired HRV were identified. In thosecases, mortality was as high as 50% over 5
evidence that caffeine caused cardiac dys-
years (12). In our study, patients with se-
rhythmia or tolerance (attenuation of the
cause the disease process associated with
this may be associated with a reduction in
reversibly. This highlights the importance
of identifying and treating patients at risk
sympathetic and parasympathetic tracts.
lier in an attempt to improve cardiovascu-
function tests may identify individuals at
is likely to be of potential benefit to car-
tality (12), HRV appears to be a sensitivemarker of autonomic dysfunction at anearlier stage (13,14). In our study, weused sNN50 per hour as a measure ofHRV. This is considered to be a thresholdbeyond which each RR interval must passin order to be counted and has been sug-gested to be the most sensitive test for thedetection of diabetic autonomic neuropa-thy (15). A reduction in HRV indicatesincreased cardiovascular risk indepen-dently of traditional coronary risk factors(16).
differentiate the various components ofsympathovagal activity on HRV. In thisstudy, the HF domain was used as amarker of parasympathetic activity, andthe LF-to-HF ratio was used as a mea-sure of sympathetic activity (17). Impair-ment in parasympathetic function withrelative sympathetic overactivity pre-disposes to ventricular dysrhythmias
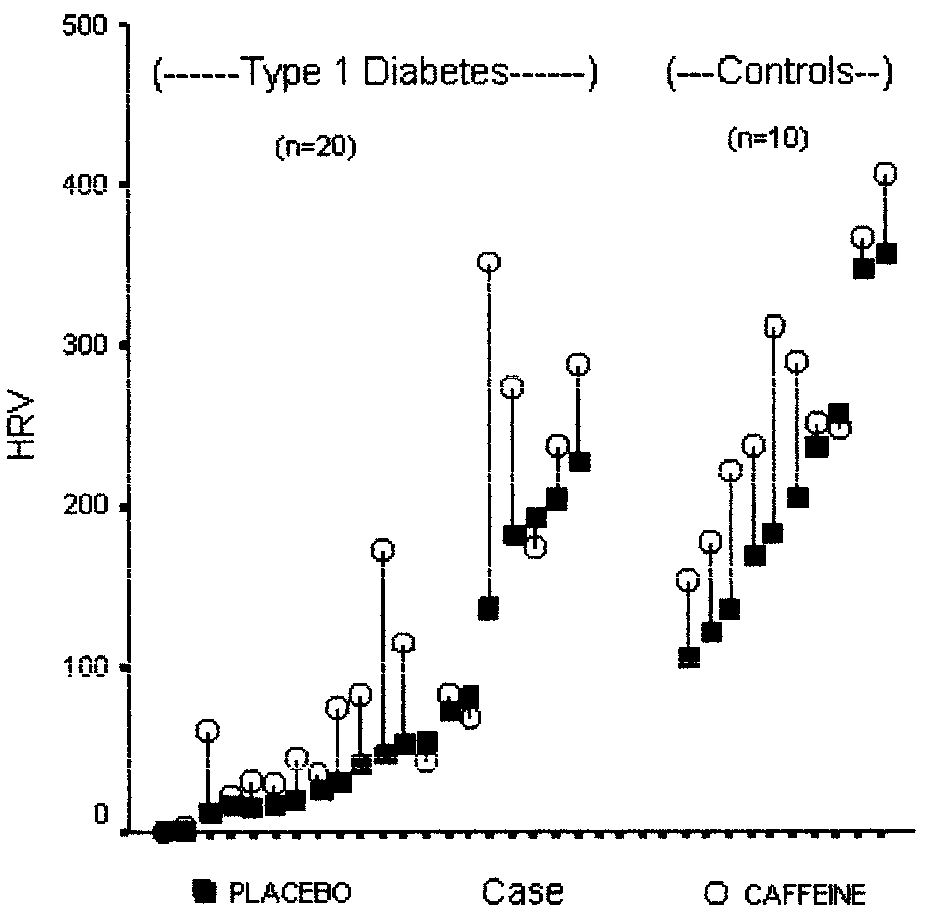
Figure 2—Absolute change in HRV with caffeine in patients with type 1 diabetes and in control
DIABETES CARE, VOLUME 27, NUMBER 5, MAY 2004
Caffeine and heart rate variability Table 2—Influence of caffeine on HRV (time domain and spectral analysis) in type 1 diabetic and control subjects
diovascular health, as there is no evidence
of heart rate variability to identify patients
of a cutoff for HRV-associated cardiovas-
at risk. Cardiovasc Res 50:210 –217, 2001
11. Task Force of the European Society of
cular morbidity. The benefit of caffeine is
that it is readily available to the majority
Heart rate variability: standards of mea-
risk of coronary heart disease in the gen-
and clinical use. Eur Heart J 17:354 –381,
eral population. J Intern Med 248:483–
world. A cup of percolated coffee contains
4. Watson JM, Jenkins EJ, Hamilton P, Lunt
a cup of filter coffee contains 142 mg (25).
nostic implications. Ann Intern Med 92:
In patients with cardiac disease, coffee has
mia in free-living patients with type 1 di-
abetes. Diabetes Care 23:455– 459, 2000
13. Sega S, Jager F, Kiauta T: A comparison of
time in the atrioventricular node (26) but
5. Watson JM, Sherwin RS, Deary IJ, Scott L,
not to predispose to ventricular dysrhyth-
analysis of heart rate variability in healthy
mias following myocardial infarction. The
subjects. Clin Auton Res 3:175–182, 1993
majority of studies have found no associ-
14. Ziegler D, Gries FA, Muhlen H, Rathmann
caffeine use. Clin Sci (Lond) 104:447– 454,
clinical correlates of cardiovascular auto-
6. Debrah K, Haigh R, Sherwin R, Murphy J,
thy in patients attending diabetes centers:
doses resembling average daily coffee in-
feine use on the cerebrovascular, cardio-
the Diacan Multicenter Study Group. Dia-
orthostasis in healthy volunteers. Clin Sci
whether caffeine may be associated with a
7. Mastrototaro JJ: The MiniMed continuous
thetic activity using 24 hour electrocar-
glucose monitoring system (CGMS). J Pe-
diograms. Br Heart J 52:396 – 402, 1984
diatr Endocrinol Metab 12:751–758, 1999
16. Wheeler SG, Ahroni JH, Boyko EJ: Pro-
8. Ewing DJ, Neilson JM, Shapiro CM, Stew-
as a predictor of mortality in patients with
rate variability: effects of posture, sleep
diabetes. Diabetes Res Clin Pract 58:131–
Acknowledgments — This study was sup-
ported by an educational grant from the Coffee
Science Information Centre. The sponsors had
nomic function in diabetic patients. Br
variability: basic studies. In Heart Rate
no role in study design, data collection, anal-
Variability. Malik M, Camm AJ, Eds. Ar-
ysis, or interpretation, or the decision to sub-
9. Albrecht P, Cohen RJ: Estimation of heart
18. Singh N, Mironov D, Armstrong PW, Ross
world data: dealing with ectopic beats and
AM, Langer A: Heart rate assessment early
noisy data. Comput Cardiol 15:311–314,
after acute myocardial infarction. Circula-References
1. Villareal RP, Liu BC, Massumi A: Heart
19. Manfrini O, Pizzi C, Trere D, Fontana F,
rate variability and cardiovascular mortal-
Bugiardini R: Parasympathetic failure and
ity. Curr Atheroscler Rep 4:120 –127, 2002
Efficient estimation of heart period power
risk of subsequent coronary events in un-
2. Lombardi F, Makikallio TH, Myerburg RJ,
pharmacologic studies. Am J Cardiol 66:
tion myocardial infarction. Eur Heart J 24:
DIABETES CARE, VOLUME 27, NUMBER 5, MAY 2004
Richardson and Associates
diabetes mellitus. J Intern Med 246:299 –
20. Pagnani M, Malfatto G, Pierini S, Casti R,
25. Bunker ML, McWilliams M: Caffeine con-
Cerutti S, Malliani A: Spectral analysis of
nomic neuropathy. Diabet Med 7:105–
tent of common beverages. J Am Diet Assoc
heart rate variability in the assessment of
autonomic neuropathy. J Auton Nerv Syst
23. Marques JL, George E, Peacey SR, Harris
of coffee in man. J Clin Pharmacol 19:46 –
diabetes. Diabet Med 14:648 – 654, 1997
27. Chou TM, Benowitz NL: Caffeine and cof-
24. Landstedt-Hallin L, Englund A, Adamson
fee: effects on health and cardiovascular
ropathy in diabetes mellitus. Diabetes
disease. Comp Biochem Physiol C Pharma-
ing hypoglycaemia in patients with type 2
col Toxicol Endocrinol 109:173–189, 1994
DIABETES CARE, VOLUME 27, NUMBER 5, MAY 2004
1. What is a change in the number of entire chromosome sets called?a. Aneuploidyb. Euploidyc. Monosomyd. Trisomye. Deficiency2. What is an individual with only one set (n) of chromosomes called?a. Triploidb. Monosomicc. Trisomicd. Haploide. Polyploid3. Bread wheat is an allohexaploid. What is its most likely origin?a. Tripling the original diploid number by use of colchicineb. Crossing with o
6. Literaturverzeichnis Akaike T, Suga M, Maeda H ( 1998 ): Free radicals in viral pathogenesis: molecular mechanisms involving superoxide and NO; Proc Soc Exp Biol Med 217(1): 64-73. Akama KT, Albanese C, Pestell RG, Van Eldik LJ ( 1998 ): Amyloid beta-peptide stimulates nitric oxide production in astrocytes through an NFkappaB-dependent mechanism; ProcNatl Acad Sci U S A 95(10): 5795-800.
 Richardson and Associates
Richardson and Associates