Review Article Juvenile Dermatomyositis: A Review
Geetha Chari, MD; Teresita A. Laude, MD, FAAP, FAAD
Abstract
acute and severe onset. It appears to have a seasonal predi-lection, occurring more frequently in the spring and summer
Juvenile dermatomyositis is a systemic vasculopathy, affecting
months. A history of antecedent illness is often obtained in
mainly the skin and muscle. In the United States, it is seen in more
newly diagnosed juvenile dermatomyositis. Studies impli-
than three per million children per year. It is diagnosed on the
cate Coxsackie virus on the basis of viral antibody findings
basis of the criteria set by Bohan and Peter. The following review
describes the characteristic clinical manifestations, the patho-
Juvenile dermatomyositis has a strong association with
physiology and immunology of the disease. The various treatment
the HLA antigens B8/DR3 and DQA1*0501 allele. 1
modalities are discussed. Int Pediatr. 2000;15(1):21-25.Diagnostic Criteria Key words: juvenile dermatomyositis, vasculopathy
Bohan and Peter set forth criteria for the diagnosis of juve-
nile dermatomyositis and polymyositis in childhood. These
Introduction
criteria assume that the child has the characteristic rash, afterwhich three of the four criteria must be fulfilled for definite
Juvenile dermatomyositis is a systemic vasculopathy, af-
disease, two of four for probable disease and one of four for
fecting primarily the skin and muscle, causing symmetric
proximal weakness and characteristic skin rash. It differsfrom the adult form of dermatomyositis by the presence of
Table 1.—Diagnostic Criteria For Juvenile Dermatomyositis2
vasculitis of the small blood vessels, which can involve thegastrointestinal tract and myocardium, besides skin and
Juvenile dermatomyositis Polymyositis
muscle. Calcinosis is an additional feature that is present in
juvenile dermatomyositis, but not in the adult form of der-
matomyositis. Juvenile dermatomyositis is not associated
with development of malignancies, unlike adult dermato-
Epidemiology
Electromyographic changes:Inflammatory myopathy
Juvenile dermatomyositis is the most common of the in-
flammatory myopathies of childhood, affecting about threeper million children per year.1
Clinical Features
Dermatomyositis has a bimodal distribution in the age of
onset, occurring in two peaks, one at 5 to 14 years and the
The onset of juvenile dermatomyositis is acute in 50% of
patients, with rapid development of weakness and rash.
Juvenile dermatomyositis is 10 – 20 times more common
Children who have a subacute onset may present a skin rash,
than polymyositis in children, and tends to have a more
a gradually progressive weakness of muscles, jointcontractures or difficulty using hands because of tendon in-
From the Departments of Dermatology and Pediatrics, State
volvement. The usual time period between onset of disease
symptoms and diagnosis is approximately three months. Inthose children who had only weakness as the presenting com-
Address reprint requests to Department of Dermatology (Box 46),
plaint, diagnosis could be delayed to 12 months or greater.3
450 Clarkson Avenue, Brooklyn, NY 11203 (Dr Laude)
Besides the characteristic manifestations described be-
low, children often have low-grade fever, malaise, weightloss, and poor appetite. International Pediatrics/Vol. 15/No. 1/2000
Calcinosis Cutaneous Manifestations
Soft tissue calcifications occur in up to 40% of the pa-
The rash may precede or follow the onset of proximal
tients in the late stages. Skin calcinosis is seen as crusted
muscle weakness. The characteristic rash is violaceous or
papules or plaques around joints or as nonhealing sores.
heliotropic, occurring most prominently on the eyelids (Fig-
Sometimes, the calcific material is extruded through the skin
ure 1). Periorbital edema can be seen. Eyelid telangiectasia
as a white cheesy exudate, leaving behind a dry pitted scar.
accompanies the periorbital edema in 50 – 90% of children.
Muscle calcification results in contractures or severe muscu-
Exposure to sunlight can cause exacerbation of the skin in-
lar pain. Four patterns of calcification are seen: superficial
flammation or may precipitate activation of myositis.
and deep calcarial masses, deep linear deposits (Figure 4)
Erythema can occur over the upper parts of the body (shawl
and lacy reticular subcutaneous deposition encasing the
sign) and extensor surfaces of arms and legs.
The skin over the knuckles may be hypertrophic or pale
red and evolve into atrophic bands. Gottron’s papules are
Musculoskeletal Features
flat-topped red papules on the knuckles(Figure 2).
Proximal muscle weakness is the major feature. This is
Erythematous plaques with fine scales are seen on the elbows,
manifested by difficulty in raising the arms above the shoul-
knees, and medial malleoli of the ankles. A livedo
ders, inability to comb the hair, and difficulty in climbing
reticularis pattern may be seen on the extremities. Diffuse
stairs. Neck flexor weakness is an especially sensitive indica-
vasculitis may be manifested by nailbed telangiectasia, inf-
tor of muscle weakness. Muscle pain is not a frequent symp-
arction of oral epithelium, skin folds or digital ulceration.1
tom. The child usually keeps the limbs in a flexed position,
The scalp may be involved with diffuse, scaly dermatosis
which promotes development of flexion contractures and
and often nonscarring alopecia4 (Figure 3). This is often
misdiagnosed as seborrheic dermatitis or psoriasis.
There may be difficulty in swallowing due to palatal
Panniculitis is a rare finding, where indurated plaques
muscle weakness, with regurgitation and a nasal voice. Pool-
and nodules are found mainly on the arms, thighs and but-
ing of barium in a wide atonic pyriform fossa may be seen.
tocks. These can be erythematous and painful.5
Esophageal dysfunction may be present.
Hypertrichosis is another unusual feature of juvenile der-
The myopathy may be focal, especially early in disease
matomyositis, the pathogenesis of which is not known. Hair
onset. Therefore a normal area may be erroneously targeted
growth may be more prominent on the forehead, cheeks,
in EMG or biopsy. MRI of the muscles can help detect the
forearms and legs. Hypertrichosis may respond to the steroid
Decreased bone density may be present, leading to in-
Fig 1.—Heliotrope, erythema on the face of a 10 year old with a one
Fig 2.—Gottron’s papules (same patient as in Figure 1)
International Pediatrics/Vol. 15/No. 1/2000
monly leads to asymptomatic conduction abnormalities. These resolve when disease activity subsides. Pulmonary Findings
There is a decrease in ventilatory capacity in the absence
of respiratory complaints. Pulmonary fibrosis can occur, butis more common with children who have antibodies to Jo-1. Ophthalmic Findings
Thrombosis of vessels at the eyelid margin may be seen.
“Cotton-wool” spots on the retina result from small vesselocclusion. Intraretinal edema can cause injury to the retinalnerve fibers and lead to optic atrophy and visual loss. Pathophysiology
Vascular lesions without a prominent inflammatory com-
ponent can be seen in juvenile dermatomyositis. Capillaries,venules and small arteries are damaged with deposition ofIgM, C3D and fibrin, with loss of muscle capillary networkand structural changes in the nailfold capillary bed. Theprimary lesion occurs in the endothelial cell, which containsreticulotubular inclusions that are the site of thrombosis andvessel obliteration.1
The muscle pathology reflects vascular compromise and
capillary dropout, with perivascular atrophy of both type Iand type II muscle fibers, and inflammatory infiltrates of
Fig 3.—Occipital alopecia in a child with dermatomyositis
mononuclear cells and plasma cells. CD4+ cells predomi-nate in the infiltrate, which is primarily around the bloodvessels.
Soft tissue calcification is accompanied by urinary excre-
tion of gamma-carboxyglutamic acid, which is a componentof the vitamin K dependent coagulation pathway. How-ever, no clear mechanism has been identified for the occur-rence of calcinosis. Immunology
Antinuclear antibodies, mainly of the speckled variety,
are seen in over 60% of the patients. Myositis-specific au-toantibodies are seen in about 10% of children with juveniledermatomyositis, the most common being anti-Mi2
Fig 4.—Calcinosis cutis in dermatomyositis (courtesy of Guinter
antibody(Table 2). Von Willebrand factor (vWF) released
from the damaged endothelial cells was noted to be in-
Gastrointestinal Symptoms
creased in active juvenile dermatomyositis in various stud-
Decreased esophageal motility leads to difficulty in han-
dling secretions. Involvement of the masseter can lead to
Serum levels of neopterin, a pteridine derived from acti-
difficulty in chewing food. Vasculitis leading to mucosal
vated macrophages, is elevated in about 60% of patients and
ulcerations may result in frank bowel perforation, which can
correlates with clinically active disease.
Studies have also shown that absolute lymphocyte counts
were low in active juvenile dermatomyositis, but the per-
Cardiac Abnormalities
centage of B lymphocyte counts were significantly increased,
Abnormalities in EKG are seen in over half the children
with an increase in CD4/CD8 ratio, and this reverted only
with juvenile dermatomyositis. Myocarditis most com-
International Pediatrics/Vol. 15/No. 1/2000
Table 2.—Myositis Associated Antibodies8 Table 3.—Laboratory Features2 Anti-synthetase autoantibodies Anti-Mi-2 autoantibodies Anti-signal recognition particle autoantibodies Anti-SRP Other myositis-specific autoantibodies
Myositis without any of the above autoantibodies
MRI Studies
MRI is useful in identifying areas of involvement, which
Residual disability is related mainly to calcification and
is detected by positive T2 images. Studies have shown that
MRI detects areas of involved muscle in those children withnormal muscle enzymes. MR spectroscopy using P31 can be
Treatment
used to monitor response to therapy, when other indicatorshave normalized.
Corticosteroids are the mainstay of therapy for children
One must however remember that MRI images are not
specific to juvenile dermatomyositis. Similar changes can be
With severe vasculitis, IV methylprednisolone at the dose
seen in inflammatory myopathies, strenuous exercise, a pro-
of 30 mg/kg (max. 1 gm) can be given every other day untill
the muscle enzymes and vWF have returned to normal. Then oral therapy with prednisone is started at a dose of 2
Electromyography
mg/kg/day. In most cases, improvement is seen over the first4 weeks of steroid treatment. After this, the dose of oral
EMG shows changes suggestive of myopathy. However, it
steroids is gradually reduced and changed to an alternate day
can be negative in up to 10% of new onset juvenile dermato-
regimen. Monitoring the patient for the adverse effects of
myositis despite elevated muscle enzymes, due to improper
electrode placement into normal areas of muscle.
If the skin rash is very prominent, hydroxychloroquine
(up to 7 mg/kg/day) is started, along with topical steroids and
Prognosis
lubricants. Use of sunscreen (SPF 16 or more) will reduceexposure to UV light, so as to decrease disease activation.
Prognosis is related to the degree of vasculitis. Death can
Presence of myocarditis, persistent dysphagia, diplopia
occur in the acute phase due to myocarditis, progressive un-
and dyspnea, especially with weakness of intercostal muscles
responsive myositis or occasionally due to lung involvement
suggests bad prognostic features. In these children, early
or bowel perforation secondary to ulceration. Infection dur-
therapy with cyclosporine or cytotoxic drugs is desirable.
ing the course of intensive therapy may also result in death.
Cyclosporine A can be given in at a dose of 6 – 8 mg/kg
The clinical course can be monocyclic, chronic polycy-
clic and chronic continuous. The overall prognosis for sur-
Cytotoxic therapy is considered in those children who
vival is improved following better use of corticosteroids.
cannot be maintained on reasonable doses of steroids, with
The clinical course can be monocyclic, chronic polycy-
or without cyclosporine, or who have late vasculitis. Aza-
clic and chronic continuous. The overall prognosis for sur-
thioprine, 2.3 mg/kg/day, given orally or methotrexate given
vival is improved following better use of corticosteroids.
orally or parenterally may be tried. Short courses of cyclo-phosphamide with mesna (2-mercaptoethanesulfonic acid)
International Pediatrics/Vol. 15/No. 1/2000
may be used in presence of severe vasculitis.7
Pachman LM. Juvenile dermatomyositis: A Clinical Overview. Pediatrics in Review1990 Oct, Vol 12, No 4.
IV gammaglobulin has been given with some success in
Pachman LM, Hayford JP, Chung A, et al. Juvenile dermatomyositis at diagnosis:
anecdotal cases. IVIG was used in the form of monthly infu-
clinical characteristics of 79 children. J Rheumatol 1998, 25(6): 1198-1204.
sions of 2 gm/kg/month in those patients who did not re-
Kasteler JS, Callen JP. Scalp involvement in dermatomyositis. JAMA 1994,272:1939-1941.
spond to the traditional line of treatment.11
Ghali FE, Reed AM, Groben PA, McCaufiffe DP. Panniculitis in juvenile dermato-
Once inflammation subsides, it is important to start
myositis. Pediatr Dermatol 1999, 16(4): 270-272.
Pope DN, Strimling RB, Mallory SB. Hypertrichosis in juvenile dermatomyositis. J
muscle-training exercises. Foot drop must be prevented by
Am Acad Dermatol 1994, 31:383-387.
Ansell BM. Juvenile dermatomyositis. Rheum Dis Clin North Am 1991, 17(4):931-942.
Acute pain due to calcinosis may be treated with in-
Pachman LM. Juvenile dermatomyositis: new clues to diagnosis and pathogenesis.
domethacin or colchicine. As the disease becomes inactive
Clin & Exptl Rheumatol 1994, 12(Suppl 10): S69-S73.
and the patient is mobilized, it tends to improve. In some
Paller SA. The use of pulse corticosteroid therapy for juvenile dermatomyositis. Pediatr Dermatol 1996, 13(4): 347-348.
patients, however, it may be intractable. Surgical removal
10. Zeller V, Cohen P, Prieur A, Guillevin L. Cyclosporin A therapy in refractory juvenile
may be done in solitary subcutaneous lesions. Some reports
dermatomyositis. Experience and long term follow up of 6 cases. J Rheumatol 1996,23(8):1424-1427.
have suggested that aluminium hydroxide may be effective
11. Roifman CM. Use of intravenous immune globulin in the therapy of children with
rheumatological diseases. J Clin Immunology 1995, 15(6): Nov Suppl 42S-51S.
12. Nakagawa T, Takaiwa T. Calcinosis cutis in juvenile dermatomyositis responsive to
References
aluminium hydroxide treatment. J Dermatol 1993 Sept, 20(9): 558-560.
Pachman LM. An update on juvenile dermatomyositis. Current Opin in RheumatolInternational Pediatrics/Vol. 15/No. 1/2000
Venta y publicidad de medicamentos por Internet y la necesidad de una regulación homogénea Joaquín Catalán Socio Responsable del Área de Economía y Derecho Farmacéutico Marta Brosa Departamento Mercantil y Derecho Farmacéutico LA GACETA DE LOS NEGOCIOS. 7 de octubre de 2004 El hábito en el consumo de medicamentos está cambiando al igual que las exigencias de la demanda d
Public Liability Policy 59.CLP.5902423 Zurich Insurance Company Ltd ("the Insurer") in consideration of the Insured having paid or agreed to pay the premium and on the basis of any information provided in connection with a proposal made to the Insurer WILL SUBJECT TO THE TERMS CONDITIONS ENDORSEMENTS AND LIMITS OF INDEMNITY OF THIS POLICY INDEMNIFY THE INSURED AGAINST A. All su

 Calcinosis
Calcinosis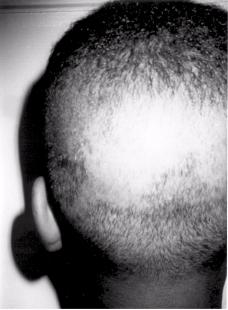
 monly leads to asymptomatic conduction abnormalities.
monly leads to asymptomatic conduction abnormalities.