One-year changes in symptoms of depression and weight in overweight/obese individuals with type 2 diabetes in the look ahead study
nature publishing group articles intervention and Prevention
One-Year Changes in Symptoms of Depression
and Weight in Overweight/Obese Individuals
Study Lucy F. Faulconbridge1, Thomas A. Wadden1, Richard R. Rubin2,3, Rena R. Wing4, Michael P. Walkup5, Anthony N. Fabricatore1, Mace Coday6, Brent Van Dorsten7, David L. Mount8, Linda J. Ewing9 and the Look AHEAD Research Group
Depressed individuals are frequently excluded from weight loss trials because of fears that weight reduction may precipitate mood disorders, as well as concerns that depressed participants will not lose weight satisfactorily. The present study examined participants in the Look AHEAD study to determine whether moderate weight loss would be associated with incident symptoms of depression and suicidal ideation, and whether symptoms of depression at baseline would limit weight loss at 1 year. Overweight/obese adults with type 2 diabetes (n = 5,145) were randomly assigned to an Intensive Lifestyle Intervention (ILI) or a usual care group, Diabetes Support and Education (DSE). Of these, 5,129 participants completed the Beck Depression Inventory (BDI) and had their weight measured at baseline and 1 year. Potentially significant symptoms of depression were defined by a BDI score ≥10. Participants in ILI lost 8.6 ± 6.9% of initial weight at 1 year, compared to 0.7 ± 4.8% for DSE (P < 0.001, effect size = 1.33), and had a reduction of 1.4 ± 4.7 points on the BDI, compared to 0.4 ± 4.5 for DSE (P < 0.001, effect size = 0.23). At 1 year, the incidence of potentially significant symptoms of depression was significantly lower in the ILI than DSE group (6.3% vs. 9.6%) (relative risk (RR) = 0.66, 95% confidence interval (CI) = 0.5, 0.8; P < 0.001). In the ILI group, participants with and without symptoms of depression lost 7.8 ± 6.7% and 8.7 ± 6.9%, respectively, a difference not considered clinically meaningful. Intentional weight loss was not associated with the precipitation of symptoms of depression, but instead appeared to protect against this occurrence. Mild (or greater) symptoms of depression at baseline did not prevent overweight/obese individuals with type 2 diabetes from achieving significant weight loss. IntroductIon
experienced adverse emotional reactions, including clinical y
Two questions frequently arise when considering whether significant depression (1). Some investigators believe that dieting
depressed, obese individuals should undertake weight reduc-
and weight loss have similar ill effects in overweight/obese indi-
tion. The first is whether dieting and weight reduction precipi-
viduals (6,7), although studies of weight loss achieved with behav-
tate (or exacerbate) symptoms of depression (1–3). The second ioral treatments have revealed reductions, rather than increases,
question is whether individuals with mild or greater symptoms in symptoms of depression (8–10). With one exception (11),
of depression can achieve the same magnitude of weight loss as previous studies have been limited by small samples and by the
obese individuals without any symptoms of depression (4,5).
failure to examine the incidence (and resolution) of symptoms of
The concern that weight loss may precipitate symptoms of depression. In addition, prior studies typical y have not included
depression arose from a study of normal weight volunteers a control group of nondieting individuals against which to judge
who lost nearly 25% of their body weight and subsequently changes in mood observed in individuals assigned to lose weight.
1Department of Psychiatry, University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania, USA; 2Department of Medicine, The Johns Hopkins University School of Medicine, Baltimore, Maryland, USA; 3Department of Psychiatry, The Johns Hopkins University School of Medicine, Baltimore, Maryland, USA; 4Department of Psychiatry and Human Behavior, Warren Alpert Medical School of Brown University, Providence, Rhode Island, USA; 5Department of Biostatistical Sciences, Wake Forest University School of Medicine, Winston-Salem, North Carolina, USA; 6Department of Preventive Medicine, The University of Tennessee Health Science Center, Memphis, Tennessee, USA; 7Department of Physical Medicine and Rehabilitation, University of Colorado School of Medicine, Aurora, Colorado, USA; 8Department of Internal Medicine, Wake Forest University School of Medicine, Winston-Salem, North Carolina, USA; 9Department of Psychiatry, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania, USA. Correspondence: Lucy F. Faulconbridge ([email protected])
Received 21 January 2011; accepted 11 September 2011; advance online publication 20 October 2011.
articles intervention and Prevention
Lack of motivation and concentration, two cardinal features Baseline demographic information is provided in Table 1. Sixty-three
of depression, could undermine efforts to adhere to rigorous percent of the sample was self-identified as non-Hispanic white, 16% as
diet and activity recommendations, and several studies have African American, 13% Hispanic, 5% American Indian, and 1% as Asian/
Pacific Islander. Forty percent of participants were male.
shown depression to be a predictor of attrition from weight loss
programs (12,13). Studies of whether pretreatment symptoms
of depression impede weight loss have yielded mixed results. Intervention
Participants were randomly assigned to ILI or DSE, both of which have
Several investigations found no relationship between these two been described previously (24,29). The ILI, modeled after the Diabetes
variables (5,13,14), while others observed smaller weight losses Prevention Program’s Lifestyle Balance intervention (30), sought to
in patients with greater pretreatment symptoms of depression induce a mean weight loss ≥7% of initial weight and to increase physical
(4,15,16). All of these studies were limited by small sample sizes activity to ≥175 min a week. Participants received intensive behavioral y
and by relatively low levels of baseline depression, the latter oriented diet and physical activity counseling during the first year. They
were provided three group and one individual meeting(s) each month
occurrence resulting from investigators’ tendency to exclude during months 1–6, and two group and one individual session(s) per
depressed individuals from weight loss trials (17–21).
month during months 7–12. Participants were instructed to consume
In the present investigation, we used data from the Look a diet of 1,200–1,800 kcal/day (based on body weight) which, during
AHEAD (Action for Health in Diabetes) study to: (i) assess the the first 4 months, included replacing two meals and one snack per day
effects of dieting and weight loss on the precipitation (and pos-
with liquid shakes and meal bars. Participants in the DSE group were
offered three group meetings during the year and were given educa-
sible resolution) of symptoms of depression; and (ii) examine tional information on nutrition, physical activity, and social support.
whether individuals with symptoms of depression at baseline
would lose less weight than individuals with no symptoms of dependent measures
depression. Look AHEAD is examining the long-term effects on Demographics and anthropometric characteristics. Weight was
cardiovascular morbidity and mortality of an Intensive Lifestyle measured at baseline and 1 year (by assessors masked to treatment con-
Intervention (ILI), compared with a usual care group, referred dition) using a digital scale (Tanita, Wil owbrook, IL, model BWB-800).
to as Diabetes Support and Education (DSE), in 5,145 over-
Height was measured at baseline using a wall-mounted stadiometer.
weight and obese individuals with type 2 diabetes. The fact that Mood and suicidal ideation. Symptoms of depression were assessed at
overweight individuals with type 2 diabetes are known to be at baseline and 1 year using the Beck Depression Inventory (BDI) (31), a
increased risk of depression (22,23) makes this an excel ent sam-
21-item questionnaire that assesses mood over the previous week. This
ple with which to address the questions outlined above.
instrument is an effective screening tool for major depression in diabetic
patients (32). Total scores range from 0 to 63, with higher values indicat-
At the end of the first year of treatment, weight losses for the ing greater symptoms of depression. In the present study, however, item
ILI and DSE groups were 8.6% and 0.7%, respectively (24). In #19, which assesses recent weight loss, was excluded from analysis because
addition, health-related quality of life (which included assess-
participants were overweight/obese and were required to be weight stable
ment of symptoms of depression) improved more in the ILI at entry. Thus, our use of the inventory yielded scores of 0–60. Scores of
than DSE groups (25). Using this data set, we compared the 0–9 reflect minimal (i.e., subclinical) symptoms, whereas values of 10–18,
19–29, and ≥30 indicate mild, moderate, and severe symptoms of depres-
incidence (as well as resolution) of symptoms of depression in sion, respectively (33). Participants who endorsed current symptoms of
the ILI and DSE groups. Given the generally favorable effects depression (i.e., scores ≥10 on the BDI) were classified as reporting mild
of weight loss on mood, we hypothesized that the ILI group or greater symptoms of depression, regardless of whether they were tak-
would show a smaller incidence of symptoms of depression ing antidepressant medication.
than those in DSE. We included an examination of suicidal
Item #9 on the BDI assesses suicidal ideation, as judged by the fol ow-
ing responses: (a) “I do not have any thoughts of killing myself;” (b) “I
ideation, given recent concerns that weight loss achieved with have thoughts of killing myself, but I would not carry them out;” (c) “I
weight loss medications (e.g., rimonabant) may precipitate would like to kill myself;” and, (d) “I would kill myself if I had the chance.”
suicidal behavior (26,27). Finally, we hypothesized that indi-
For the purpose of this study, respondents who endorsed options b, c, or
viduals in the ILI and DSE groups, who reported symptoms of d were deemed to have suicidal ideation.
depression at baseline, would achieve smaller weight losses at Binge eating. Binge-eating behavior was assessed by self-report using
1 year than would those who were free of such symptoms.
items from the Questionnaire on Eating and Weight Patterns (34). Par-
ticipants were classified as having binge-eating behavior if in the past 6
Methods and Procedures
months they reported one or more episodes of eating a large amount of
Participants
food in a discrete period of time, experienced a sense of loss of control
The Look AHEAD study design and participants have been described in
during that eating episode, and denied use of any compensatory behav-
detail previously (28). In summary, overweight/obese individuals with
iors (such as purging or excessive exercise).
type 2 diabetes were recruited from 16 clinical centers in the United
States. Participants were 45–76 years old and had a BMI ≥27 kg/m
General health and diabetes duration.
≥25 kg/m2 if on insulin). Individuals with inadequate diabetes con-
36-Item Short-Form Survey, version 2, was used at baseline to assess
trol (i.e., hemoglobin A (HbA ) >11%), or with conditions likely to
general health. The 36-Item Short-Form Survey is a well-validated mea-
affect treatment adherence, safety, or retention, were excluded from the
sure of health-related quality of life (35). At baseline, participants also
trial. Individuals diagnosed with psychosis or bipolar disorder, or who
indicated the number of years since being diagnosed with diabetes.
had been hospitalized for depression in the past 6 months, also were
excluded. Al participants provided informed consent, as approved by
statistical analyses
each site’s institutional review board.
Al analyses were performed using SAS statistical software, version 9.2
The present analysis was based on 5,129 participants who enrolled
(SAS Institute, Cary, NC). Mean values (±s.d.) are reported. Differences
in the study and completed baseline assessments of weight and mood.
in demographic variables between participants with symptoms of
www.obesityjournal.org articles intervention and Prevention
depression (BDI ≥10) and those without symptoms were compared
Differences in changes in symptoms of depression (continuous scores
using linear regression models (with gender and clinical site as covari-
on the BDI) between participants with and without symptoms of depres-
ates) for continuous variables. Generalized linear models with a multi-
sion at baseline, and between ILI and DSE groups, were compared using a
variate distribution were used for categorical variables.
two-way ANOVA, controlling for the baseline weight, BDI score, gender,
In order to examine incidence and resolution of symptoms of depression
age, race, years of education, BED status, general health score and clinical
after 1 year of treatment, we classified each of the ILI and DSE participants
site. In order to determine the effects of baseline symptoms of depression,
into the fol owing four categories based on a BDI score of 10 or above: (i)
1-year symptoms of depression, and treatment group on weight loss at 1
participants with minimal symptoms of depression at baseline and also
year, a 2 × 2 × 2 (baseline symptoms of depression by 1-year symptoms
minimal symptoms at 1 year; (ii) individuals with minimal symptoms at
of depression by treatment group) ANOVA was conducted.
baseline but who endorsed mild or greater symptoms of depression at 1
year; (iii) participants who reported mild or greater symptoms of depres-
sion at baseline but denied symptoms at 1 year; and (iv) individuals who
Baseline characteristics
reported mild or greater symptoms of depression at baseline and also at
Demographic characteristics for participants with and without
1 year. The percentages of participants in each group who met criteria for
symptoms of depression are presented in Table 1. Participants
inclusion in each category were compared using χ2-tests.
with BDI scores ≥10 at baseline were significantly younger,
table 1 Baseline characteristics of all participants (N = 5,129), and by depression status at baseline (as determined by BdI score) Variable
Numbers (and percentages within each category) of participants are presented. For general health score and diabetes duration variables, means (±s.d.) are presented. P values indicate whether there were significant differences between participants with a BDI score <10, compared with ≥10.
BDI, Beck Depression Inventory; BED, binge-eating disorder. articles intervention and Prevention
reported fewer years of education, and were more likely to be participants with symptoms of depression at baseline (17.9%
female and to be nonwhite than those with scores <10. They vs. 16.6%) or in the number of cases of suicidal ideation
also had a significantly higher BMI, were more likely to report (SI: 2.9% vs. 2.1%, respectively). All participants with SI
bingeing behavior, and reported poorer general health scores
than participants without symptoms of depression. No differ-
endorsed the statement, “I have thoughts of killing myself,
ences in diabetes duration were found between participants but I would not carry them out.” No one reported the more
with and without symptoms of depression.
serious options, indicating desire or intent to kill themselves.
Across the whole sample, significantly more participants
Mean BDI scores for participants by treatment group and with a BDI score ≥10 (i.e., with mild or greater symptoms
depression status are presented in Table 2. The numbers of depression) endorsed suicidal ideation at baseline than
(and percentages) of participants reporting minimal, mild, among those with a score <10 (i.e., minimal symptoms of
moderate and severe symptoms of depression at baseline depression) (11.1% vs. 0.7%, relative risk (RR) = 15.8, 95%
and 1 year are depicted in Table 3. There were no signifi-
confidence interval (CI) = 10.6, 23.1; P < 0.001).
cant differences between ILI and DSE in the percentages of
Noncompleters. Of the 5,129 participants, 327 did not complete
table 2 Mean (±s.d.) baseline Beck depression Inventory
BDIs at 1 year, yielding a sample of 4,802 for the incidence
(BdI) scores for participants in the Intensive lifestyle
study. Noncompleters had a higher baseline BDI score than
Intervention (IlI) and diabetes support and education (dse)
participants who completed the 1-year assessment (6.6 ± 5.8
vs. 5.4 ± 4.8, respectively, (P < 0.001, effect size = 0.24)), with
mean scores for both groups indicating minimal symptoms of
depression. Within the ILI, 30.8% (41/133) of noncompleters
reported mild or greater symptoms of depression, compared
with 22.2% (43/194) in DSE (ns). Among participants who
completed the 1-year assessment, 16.7% (801/4,802) reported
symptoms of depression at baseline, compared to 83.3%
(4,001/4,802) who reported no symptoms (P < 0.001). No
other baseline differences were observed between participants
who did and did not complete the 1-year assessment. changes in BdI scores at 1 year
Participants in ILI showed a mean reduction in BDI score of
1.4 ± 4.7 vs. 0.4 ± 4.5 points for the DSE group. The ANOVA
showed significant main effects on BDI score change of
treatment group (P < 0.001, effect size = 0.27) and base-
line depression (P < 0.001, effect size = 0.99), as well as a
significant interaction (P < 0.035). Changes in BDI scores
table 3 numbers (and percentages) of participants with Beck depression Inventory (BdI) scores indicating minimal, mild, moderate, and severe symptoms of depression, respectively, at baseline and 1 year in the Intensive lifestyle Intervention (IlI) and diabetes support and education (dse) groups BDI category (score range)
aAt 1 year, 133 participants in the ILI group, and 194 participants in the DSE group (327 total), had missing BDI values. www.obesityjournal.org articles intervention and Prevention
symptoms of depression; 60.8% and 55.6% of ILI and DSE
participants, respectively, reported symptoms of depression
at baseline but not at 1 year (P = 0.140).
The mean BDI score for individuals who reported incident
symptoms of depression was 5.8 ± 2.6 at baseline, compared to
13.2 ± 4.4 at 1 year, yielding a mean increase of 7.4 points on
Incidence and resolution of suicidal ideation
Incident suicidal ideation was observed in ~1.4% of partici-
pants in the ILI group and 1.9% of participants in the DSE
group; these participants denied thoughts of suicide at baseline
but endorsed their occurrence at 1 year (P = 0.266). There were
no significant differences in the number of participants in ILI
and DSE who showed resolution of suicidal ideation at 1 year
(68.2% vs. 72.0%, P = 0.657). Baseline depression and changes in weight at 1 year
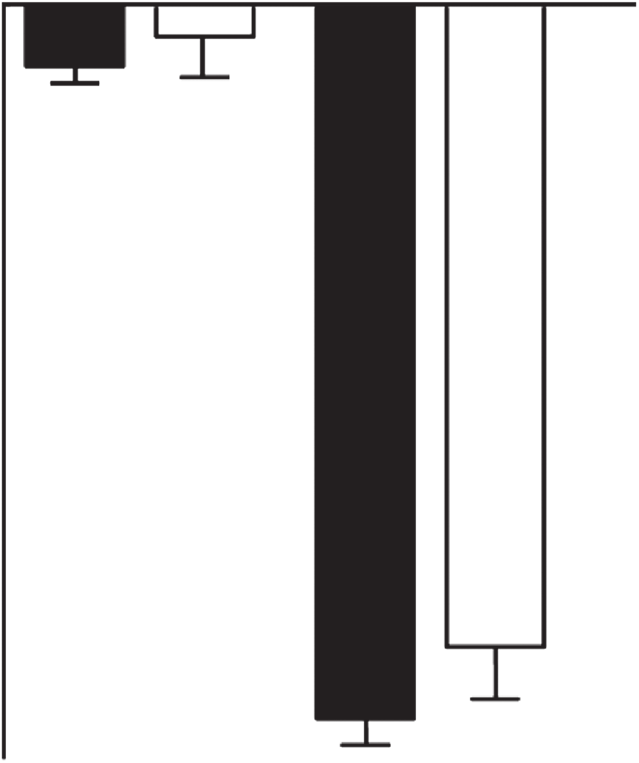
As reported previously, the ANOVA revealed a significant
main effect of weight loss on treatment group (P < 0.001,
Figure 1 Change in Beck Depression Inventory (BDI) score (±s.e.m.)
effect size = 1.23), with mean losses of 8.6 ± 6.9 and 0.7 ±
at 1 year in Intensive Lifestyle Intervention (ILI) and Diabetes Support
4.8% for ILI and DSE, respectively. A significant main effect
and Education (DSE) groups by depression status at baseline. D,
of baseline symptoms of depression also was observed (P =
participants who reported symptoms of depression at baseline; ND, participants with no/minimal symptoms reported at baseline. Mean
0.009, effect size = 0.10); participants with mild or greater
(±s.d.) baseline BDI scores were as follows: ILI-ND 3.6 ± 2.7; ILI-D
symptoms of depression lost 4.3 ± 7.0%, compared with 4.8
14.4 ± 4.5; DSE-ND: 3.8 ± 2.8; DSE-D: 13.5 ± 3.7.
± 7.1% for those with minimal symptoms. The treatment
group by depression status interaction was not significant
for participants in ILI and DSE who did and did not report (P = 0.110). As shown in Figure 2, within the ILI group,
symptoms of depression at baseline are shown in Figure 1. participants with minimal vs. mild or greater symptoms of
Participants within the ILI who reported baseline symp-
depression lost 7.8 ± 6.7% and 8.7 ± 6.9%, respectively, with
toms of depression showed a decline of 5.3 ± 6.8 points corresponding losses in the DSE group of 0.4 ± 5.0% and 0.7
on the BDI at 1 year, compared with a decline of 0.6 ± 3.7 ± 4.7%, respectively.
points for individuals reporting no symptoms of depression.
Participants with mild or greater symptoms of depression changes in mood category and weight at 1 year
in DSE showed a reduction of 3.7 ± 6.2 points on the BDI, Changes in weight for participants who showed incidence, res-
compared to an increase of 0.2 ± 3.8 points on the BDI for olution or maintenance of symptoms of depression are shown
in Table 4. The ANOVA revealed a significant (P = 0.006)
three-way interaction between baseline depression status,
Incidence and resolution of depression at 1 year
1-year depression status, and treatment group. Participants in
Table 4 shows frequencies of participants who acknowl-
ILI (n = 127) without symptoms of depression at baseline, but
edged mild or greater symptoms of depression (BDI ≥10) at who developed mild or greater symptoms of depression during
baseline and 1 year. At the end of the year, 6.3% of ILI par-
the year (i.e., incident), lost 4.6 ± 6.4% of initial body weight.
ticipants who did not report symptoms at baseline reported This was significantly (P < 0.001, effect size = 0.65) less than the
the onset of symptoms of depression (i.e., incident depres-
9.0 ± 6.9% lost by participants who showed resolution of their
sion), which was significantly lower than the 9.6% observed symptoms of depression (n = 254) and less than (P < 0.001,
in the DSE group (RR = 0.66, 95% CI = 0.5, 0.8; P < 0.001). effect size = 0.65) the 9.0 ± 6.8% lost by those who reported
(The lower incidence of symptoms of depression in the ILI minimal symptoms of depression at either baseline or at 1 year
group remained statistically significant when the incidence (i.e., no symptoms of depression at either time point, n = 1,885).
of antidepressant medication use in ILI and DSE (4.3% vs. ILI participants who both started and ended the study with a
2.7%, respectively) was controlled for (RR = 0.64, 95% CI = BDI score ≥10 (i.e., maintained symptoms of depression, n =
0.5, 0.8, P < 0.001).) A logistic regression analysis showed 164) lost 6.2 ± 6.0% of initial weight, which was significantly
that being assigned to DSE significantly increased the odds less than the weight lost by participants who showed resolu-
of reporting symptoms of depression at 1 year (odds ratio = tion (P < 0.001, effect size = 0.42), or who reported no symp-
1.62, 95% CI = 1.3, 2.1; P < 0.001). There were no signifi-
toms of depression at either time point (P < 0.001, effect size =
cant differences between ILI and DSE groups, however, in 0.42), but was not significantly different from participants who
the numbers of participants who showed resolution of their showed incident symptoms of depression (P > 0.05). articles intervention and Prevention table 4 changes in depression status at 1 year, and corresponding changes in weight and Beck depression Inventory (BdI) score, for participants in the Intensive lifestyle Intervention (IlI) and diabetes support and education (dse) groups
Incident depression is shown by persons who reported minimal symptoms of depression at baseline but reported mild or greater symptoms by 1 year. Resolution of depression is shown by persons who reported mild or greater symptoms of depression at baseline but reported minimal symptoms at 1 year. Negative numbers indicate decreases in weight or BDI score.
Participants who both started and ended the study with a BDI
score ≥10 (i.e., maintained, n = 170) gained 0.4 ± 4.7% of their
initial weight. Participants in DSE who maintained symptoms of
depression lost significantly less weight than those who showed
resolution of their symptoms of depression (P = 0.003, effect size
= 0.31), those who showed no symptoms of depression at either
baseline or at 1 year (P = 0.002, effect size = 0.25), and partici-
pants who showed incident symptoms of depression at year 1
(P = 0.017, effect size = 0.25). There were no other statistical y
significant differences among the other three groups. Psychiatric adverse events
Adverse psychiatric events were reported on an ad hoc basis.
During the year, five participants reported an adverse event
involving depression; three of these cases were in the ILI group
and two were in the DSE group. None of these events involved
suicidal behavior. Of these five participants, none reported
symptoms of depression at baseline (defined by BDI ≥10), but
three participants reported use of antidepressant medication
Figure 2 Mean percent (±s.e.m.) of initial weight lost at 1 year in Intensive Lifestyle Intervention (ILI) and Diabetes Support and Education (DSE) groups by depression status at baseline. D, participants who dIscussIon
reported mild or greater symptoms of depression at baseline; ND,
This is the first randomized controlled trial of which we are
participants with no/minimal symptoms reported at baseline.
aware to examine precipitation and resolution of symptoms
A 2 × 2 ANOVA (i.e., treatment-group by depression-status) revealed
of depression in individuals who received a lifestyle modifi-
that ILI participants lost significantly (P < 0.001) more weight than DSE participants and that participants considered free of symptoms
cation weight loss intervention, compared with participants
of depression at baseline lost significantly (P < 0.009) more weight
in a nondieting control group. At 1 year, participants in the
than those who reported mild or greater symptoms of depression. The
ILI lost a mean of 8.6% of their initial weight, compared to
treatment group by depression status interaction was not significant
0.7% for those in DSE (24), and reported significantly greater
improvements in symptoms of depression compared with DSE
participants (1.4 vs. 0.4 points) (25). Participants in ILI with
Participants in the DSE group who showed incident symp-
baseline BDI scores ≥10 showed an even larger reduction of 5.3
toms of depression (n = 190) lost 0.7 ± 5.2% of initial weight, points, compared to 0.6 for those without baseline symptoms
whereas those who showed no symptoms of depression at either of depression. These findings suggest that moderate weight loss
baseline or at 1 year (n = 1,799) lost 0.7 ± 4.6%, and those who in patients with mild to moderate symptoms of depression is
showed resolution of their depression (n = 213) lost 1.0 ± 5.1%. associated with improvements, not worsening, in mood. www.obesityjournal.org articles intervention and Prevention
In the present study, we observed a significantly lower number weight and achieve improvements (rather than worsening) in
of incident cases of symptoms of depression in the ILI group at mood. We tentatively conclude that such individuals can be
1 year than in the DSE group (6.3% vs. 9.6%), which remained safely encouraged to lose weight and should not be routinely
significant after controlling for incident use of antidepressant excluded from weight loss trials, as currently practiced.
medications in the two groups. Individuals who reported inci-
While the presence of pretreatment symptoms of depres-
dent symptoms of depression reported a mean increase of >7 sion does not appear to substantially hamper weight loss, the
points on the BDI, which is regarded as a clinically significant onset of symptoms of depression may impede weight loss. ILI
change by experts (36). These results counter the notion that individuals who developed symptoms of depression during the
intentional dieting, with its resulting weight loss, precipitates year (i.e., cases of incident symptoms of depression) lost sig-
depression in overweight or obese individuals. Furthermore, nificantly less weight (4.6%) than those who resolved (9.0%),
the incidence of suicidal ideation at 1 year was not significantly or did not report symptoms of depression at either time point
different between participants in the ILI and DSE groups (1.4% (9.0%), and nominally less than those who maintained symp-
vs. 1.9%), suggesting that moderate weight loss resulting from toms of depression (6.2%). Thus, it appears that the presence
lifestyle change does not precipitate suicidal thoughts in this of mild or greater symptoms of depression at baseline is not
a good predictor of weight loss in a clinical trial; rather the
The DSE group provides useful information about changes presence of symptoms of depression at the end of treatment
in mood that can be expected in overweight persons (with type (regardless of whether they were present at baseline) may indi-
2 diabetes) who are not in a weight loss program. As a group, cate poorer outcomes, with the poorest for those who show
DSE participants who reported mild or greater symptoms of incident symptoms of depression. This finding is similar to that
depression at baseline showed improvements in mood at 1 obtained recently by Gorin et al. (40), who determined that
year (as indicated by a 3.7 point decline on the BDI). As noted, the presence of binge-eating behavior in Look AHEAD par-
9.6% of participants reported the onset of clinically signifi-
ticipants at baseline alone did not predict poor weight loss out-
cant symptoms of depression during the year, whereas 55.6% comes. Instead, weight loss was poorest in those participants
of those with symptoms of depression at baseline experienced who either developed bingeing behavior during the study or
remission of this condition (i.e., BDI <10). These results indi-
did not resolve their pre-existing binge-eating behavior. The
cate that mood was subject to fluctuation over the course of present study was not designed to assess causality; thus, we can-
a year in a sample of overweight individuals who were not not determine definitively whether individuals who reported
instructed to lose weight and who remained relatively weight incident symptoms of depression lost less weight because they
stable. Similar fluctuations in symptoms of depression, as well developed symptoms of depression, or whether symptoms of
as in the use of antidepressant medications, were reported over depression developed in response to achieving a smaller-than-
time in participants in the Diabetes Prevention Program (11). desired weight loss (or even partial regain of initial weight loss
Such results set the bar by which to compare changes in mood in year 1). Further studies that include more frequent assess-
associated with various weight loss interventions, including ment of both mood and weight are needed to identify the
behavioral and pharmacologic approaches. The greater reduc-
nature of the relationship between these two variables.
tion in BDI scores observed in individuals reporting symptoms
We observed comparable attrition rates between individu-
of depression at baseline in the ILI group (−5.3) vs. the DSE als with and without symptoms of depression, contrary to sug-
group (−3.7) suggests that the behavioral weight loss program gestions that depressed individuals are less likely to complete
augmented the spontaneous improvements in mood that were weight loss trials than their nondepressed counterparts. Across
observed in the DSE group at 1 year.
the sample, of the 4,802 individuals who completed the 1-year
The second aim of our study was to examine whether indi-
assessment, only 16.7% reported symptoms of depression
viduals who reported symptoms of depression at baseline at baseline, compared to 83.3% who reported no symptoms.
would lose less weight than those without such symptoms. There was no significant difference in the number of noncom-
Collapsing across the ILI and DSE groups, participants with pleters who reported mild or greater symptoms of depression
mild or greater symptoms of depression at baseline lost sig-
at baseline in the ILI vs. DSE groups (30.8% vs. 22.2%, n.s.),
nificantly less weight than individuals with no symptoms of indicating that the ILI did not increase the likelihood of indi-
depression (4.3% vs. 4.8%), but the difference cannot be con-
viduals with baseline symptoms of depression dropping out of
sidered clinically meaningful. Similarly, the difference in mean the study.
weight loss between participants with and without symptoms
The prevalence of suicidal ideation, as assessed by a single
of depression in the ILI (7.8% vs. 8.7%) is not clinically mean-
item on the BDI, was very low at baseline; only 129 of 5,129
ingful. Thus, our results do not support the routine exclusion participants (2.5%) endorsed passive suicidal thoughts. These
of participants with symptoms of depression from weight individuals were more likely to report mild or greater symp-
loss trials (17,18,37–39) based on the belief that they may toms of depression at baseline; one of every 10 participants
lose less weight than nondepressed individuals. Rather, these with symptoms of depression at baseline acknowledged SI at
findings indicate that individuals with mild or greater symp-
baseline. The incident rate of suicidal ideation was very low
toms of depression who enroll in a supervised weight reduc-
and was independent of treatment group (1.4% vs. 1.9% for
tion program are able to lose clinically significant amounts of ILI and DSE, respectively). Some have argued that the higher
articles intervention and Prevention
rates of SI (and symptoms of depression) associated with some LaFleur; Kim Landry; Missy Lingle; Jennifer Perault; Mandy
weight loss medications may be attributable to the effects of the Shipp, RD; Marisa Smith; Elizabeth Tucker.
greater weight loss induced by the medication (as compared
with placebo), rather than to a possible direct effect of the The University of Alabama at Birmingham. Cora E. Lewis,
medication on psychiatric function. Our results suggest that MD, MSPH (Principal Investigator); Sheikilya Thomas MPH
greater weight loss alone, as achieved by the ILI vs. DSE, is not (Program Coordinator); Monika Safford, MD (Co-investiga-
associated with increased SI or symptoms of depression.
tor); Vicki DiLil o, PhD; Charlotte Bragg, MS, RD, LD; Amy
Strengths of the present study include the large and ethni-
Dobelstein; Stacey Gilbert, MPH; Stephen Glasser, MD; Sara
cally diverse sample, and the inclusion of the DSE group that Hannum, MA; Anne Hubbel , MS; Jennifer Jones, MA; DeLa-
provided an estimate of spontaneous changes in mood over val ade Lee; Ruth Luketic, MA, MBA, MPH; Karen Marshall; L.
the course of the year in the absence of intentional dieting and Christie Oden; Janet Raines, MS; Cathy Roche, RN, BSN; Janet
weight loss. Significant limitations of the current study include Truman; Nita Webb, MA; Audrey Wrenn, MAEd.
its reliance on the BDI (a self-report questionnaire) as the pri-
mary assessment of mood, as well as the low level of symptoms Harvard Center: Massachusetts General Hospital. David M.
of depression in the sample, reflective of the extensive screen-
Nathan, MD (Principal Investigator); Heather Turgeon, RN,
ing process in which those who were deemed unfit to complete BS, CDE (Program Coordinator); Kristina Schumann, BA (Pro-
the study were excluded from the trial. Future studies should gram Coordinator); Enrico Cagliero, MD (Co-investigator);
incorporate structured clinical interviews and formal assess-
Linda Delahanty, MS, RD (Co-investigator); Kathryn Hayward,
ments of depression and suicidal ideation at baseline and at MD (Co-investigator); El en Anderson, MS, RD (Co-investi-
several times over the course of treatment. This is the Food gator); Laurie Bissett, MS, RD; Richard Ginsburg, PhD; Valerie
and Drug Administration’s current requirement for the assess-
Goldman, MS, RD; Virginia Harlan, MSW; Charles McKitrick,
ment of new weight loss medications that act upon the central RN, BSN, CDE; Alan McNamara, BS; Theresa Michel, DPT, DSc
nervous system (41). More frequent assessments of weight and CCS; Alexi Poulos, BA; Barbara Steiner, EdM; Joclyn Tosch, BA.
mood would allow determination of whether improvements
in symptoms of depression precede weight loss or are a conse-
Joslin Diabetes Center. Edward S. Horton, MD (Principal Inves-
tigator); Sharon D. Jackson, MS, RD, CDE (Program Coordina-
In summary, the present findings suggest that overweight and tor); Osama Hamdy, MD, PhD (Co-investigator); A. Enrique
obese individuals with mild or greater symptoms of depression Cabal ero, MD (Co-investigator); Sarah Bain, BS; Elizabeth
can successfully participate in a behavioral weight loss pro-
Bovaird, BSN, RN; Ann Goebel-Fabbri, PhD; Lori Lambert,
gram and should be encouraged to do so. Further research is MS, RD; Sarah Ledbury, MEd, RD; Maureen Mal oy, BS; Kerry
needed to assess the effect of such treatment in obese individu-
als who suffer from severe depression. Beth Israel Deaconess Medical Center. George Blackburn, MD,
look ahead research GrouP
PhD (Principal Investigator); Christos Mantzoros, MD, DSc
This report was prepared by the authors on behalf of the Look (Co-investigator); Kristinia Day, RD; Ann McNamara, RN.
AHEAD Research Group. Members of the research group who
participated in the recruitment, assessment, treatment, and University of Colorado Health Sciences Center. James O. Hil ,
retention of participants during the first year of the study are PhD (Principal Investigator); Marsha Mil er, MS, RD (Program
Coordinator); JoAnn Phil ipp, MS (Program Coordinator);
Robert Schwartz, MD (Co-investigator); Brent Van Dorsten,
clinical sites
PhD (Co-investigator); Judith Regensteiner, PhD (Co-investiga-
The Johns Hopkins Medical Institutions. Frederick L. Brancati,
tor); Salma Benchekroun MS; Ligia Coelho, BS; Paulette Cohrs,
MD, MHS (Principal Investigator); Jeff Honas, MS (Program RN, BSN; Elizabeth Daeninck, MS, RD; Amy Fields, MPH; Susan
Coordinator); Lawrence Cheskin, MD (Co-investigator); Green; April Hamilton, BS, CCRC; Jere Hamilton, BA; Eugene
Jeanne M. Clark, MD, MPH (Co-investigator); Kerry Stewart, Leshchinskiy;Michael McDermott, MD; Lindsey Munkwitz, BS;
EdD (Co-investigator); Richard Rubin, PhD (Co-investigator); Loretta Rome, TRS; Kristin Wal ace, MPH; Terra Worley, BA.
Jeanne Charleston, RN; Kathy Horak, RD. Baylor College of Medicine. John P. Foreyt, PhD (Principal
Pennington Biomedical Research Center. George A. Bray, MD
Investigator); Rebecca S. Reeves, DrPH, RD (Program Coor-
(Principal Investigator); Kristi Rau (Program Coordinator); dinator); Henry Pownal , PhD (Co-investigator); Ashok
Al ison Strate, RN (Program Coordinator); Brandi Armand, Balasubramanyam, MBBS (Co-investigator); Peter Jones, MD
LPN (Program Coordinator); Frank L. Greenway, MD (Co-
(Co- investigator); Michele Burrington, RD; Chu-Huang Chen,
investigator); Donna H. Ryan, MD (Co-investigator); Donald MD, PhD; Al yson Clark, RD; Mol y Gee, MEd, RD; Sharon
Wil iamson, PhD (Co-investigator); Amy Bachand; Michel e Griggs; Michel e Hamilton; Veronica Hol ey; Jayne Joseph, RD;
Begnaud; Betsy Berhard; Elizabeth Caderette; Barbara Cerniaus-
Patricia Pace, RD: Julieta Palencia, RN; Olga Satterwhite, RD;
kas; David Creel; Diane Crow; Helen Guay; Nancy Kora; Kel y Jennifer Schmidt; Devin Volding, LMSW; Carolyn White. www.obesityjournal.org articles intervention and Prevention University of California at Los Angeles School of Medicine.
(Co- investigator); Mary L. Klem, PhD, MLIS (Co-investigator);
Mohammed F. Saad, MD (Principal Investigator); Siran Monica E.Yamamoto, DrPH, RD, FADA (Co-investigator); Barb
Ghazarian Sengardi, MD (Program Coordinator); Ken C. Chiu, Elnyczky, MA; George A. Grove, MS; Pat Harper, MS, RD, LDN;
MD (Co-investigator); Medhat Botrous; Michel e Chan, BS; Kati Janet Krulia, RN, BSN, CDE; Juliet Mancino, MS, RD, CDE,
Konersman, MA, RD, CDE; Magpuri Perpetua, RD.
LDN; Anne Mathews, MS, RD, LDN; Tracey Y. Murray, BS; Joan
R. Ritchea; Jennifer Rush, MPH; Karen Vujevich, RN-BC, MSN,
The University of Tennessee Health Science Center: University of Tennessee East. Karen C. Johnson, MD, MPH (Principal Inves-
tigator); Carolyn Gresham, RN (Program Coordinator); Stepha-
The Miriam Hospital/Brown Medical School. Rena R. Wing, PhD
nie Connel y, MD, MPH (Co-investigator); Amy Brewer, RD, (Principal Investigator); Renee Bright, MS (Program Coor-
MS; Mace Coday, PhD; Lisa Jones, RN; Lynne Lichtermann, RN, dinator); Vincent Pera, MD (Co-investigator); John Jakicic,
BSN; Shirley Vosburg, RD, MPH; and J. Lee Taylor, MEd, MBA.
PhD (Co-investigator); Deborah Tate, PhD (Co-investigator);
Amy Gorin, PhD (Co-investigator); Kara Gal agher, PhD (Co-
University of Tennessee Downtown. Abbas E. Kitabchi, PhD, MD
investigator); Amy Bach, PhD; Barbara Bancroft, RN, MS; Anna
(Principal Investigator); Helen Lambeth, RN, BSN (Program Bertorel i, MBA, RD; Richard Carey, BS; Tatum Charron, BS;
Coordinator); Debra Clark, LPN; Andrea Crisler, MT; Gracie Heather Chenot, MS; Kimberley Chula-Maguire, MS; Pamela
Cunningham; Donna Green, RN; Debra Force, MS, RD, LDN; Coward, MS, RD; Lisa Cronkite, BS; Julie Currin, MD; Mau-
Robert Kores, PhD; Renate Rosenthal PhD; Elizabeth Smith, MS, reen Daly, RN; Caitlin Egan, MS; Erica Ferguson, BS, RD; Linda
RD, LDN; and Maria Sun, MS, RD, LDN; and Judith Soberman, Foss, MPH; Jennifer Gauvin, BS; Don Kieffer, PhD; Lauren Les-
sard, BS; Deborah Maier, MS; JP Massaro, BS; Tammy Monk,
MS; Rob Nicholson, PhD; Erin Patterson, BS; Suzanne Phelan,
University of Minnesota. Robert W. Jeffery, PhD (Principal Inves-
PhD; Hollie Raynor, PhD, RD; Douglas Raynor, PhD; Natalie
tigator); Carolyn Thorson, CCRP (Program Coordinator); John Robinson, MS, RD;Deborah Robles; Jane Tavares, BS.
P. Bantle, MD (Co-investigator); J. Bruce Redmon, MD (Co-
investigator); Richard S. Crow, MD (Co-investigator); Scott The University of Texas Health Science Center at San Antonio. Ste-
Crow, MD (Co-investigator); Susan K Raatz, PhD, RD (Co-in-
ven M. Haffner, MD (Principal Investigator); Maria G. Montez,
vestigator); Kerrin Brelje, MPH, RD; Carolyne Campbell; Jeanne RN, MSHP, CDE (Program Coordinator); Carlos Lorenzo, MD
Carls, MEd; Tara Carmean-Mihm, BA; Emily Finch, MA; Anna (Co-investigator).
Fox, MA; Elizabeth Hoelscher, MPH, RD, CHES; La Donna
James; Vicki A. Maddy, BS, RD; Therese Ockenden, RN; Birgitta University of Washington/VA Puget Sound Health Care System.
I. Rice, MS, RPh CHES; Tricia Skarphol, BS; Ann D. Tucker, BA; Steven Kahn MB, ChB (Principal Investigator); Brenda Mont-
Mary Susan Voel er, BA; Cara Walcheck, BS, RD.
gomery, RN, MS, CDE (Program Coordinator); Robert Knopp,
MD (Co-investigator); Edward Lipkin, MD (Co-investigator);
St. Luke’s Roosevelt Hospital Center. Xavier Pi-Sunyer, MD (Prin-
Matthew L. Maciejewski, PhD (Co-investigator); Dace Trence,
cipal Investigator); Jennifer Patricio, MS (Program Coordina-
MD (Co-investigator); Terry Barrett, BS; Joli Bartel , BA; Diane
tor); Stanley Heshka, PhD (Co-investigator); Carmen Pal, MD Greenberg, PhD; Anne Muril o, BS; Betty Ann Richmond, MEd;
(Co-investigator); Lynn Al en, MD; Diane Hirsch, RNC, MS, April Thomas, MPH, RD. Southwestern American Indian Center, Phoenix, Arizona and University of Pennsylvania. Thomas A. Wadden, PhD (Principal
Shiprock, New Mexico. William C. Knowler, MD, DrPH (Princi-
Investigator); Barbara J. Maschak-Carey, MSN, CDE (Program pal Investigator); Paula Bolin, RN, MC (Program Coordinator);
Coordinator); Stanley Schwartz, MD (Co-investigator); Gary D. Tina Kil ean, BS (Program Coordinator); Cathy Manus, LPN
Foster, PhD (Co-investigator); Robert I. Berkowitz, MD (Co-
(Co-investigator); Jonathan Krakoff, MD (Co-investigator);
investigator); Henry Glick, PhD (Co-investigator); Shiriki K. Jeffrey M. Curtis, MD, MPH (Co-investigator); Justin Glass,
Kumanyika, PhD, RD, MPH (Co-investigator); Johanna Brock; MD (Co-investigator); Sara Michaels, MD (Co-investigator);
Helen Chomentowski; Vicki Clark; Canice Crerand, PhD; Peter H. Bennett, MB, FRCP (Co-investigator); Tina Morgan
Renee Davenport; Andrea Diamond, MS, RD; Anthony Fabrica-
(Co-investigator); Shandiin Begay, MPH; Bernadita Fal is RN,
tore, PhD; Louise Hesson, MSN; Stephanie Krauthamer-Ewing, RHIT, CCS; Jeanette Hermes, MS,RD; Diane F. Hol owbreast;
MPH; Robert Kuehnel, PhD; Patricia Lipschutz, MSN; Monica Ruby Johnson; Maria Meacham, BSN, RN, CDE; Julie Nelson,
Mul en, MS, RD; Leslie Womble, PhD, MS; Nayyar Iqbal, MD.
RD; Carol Percy, RN; Patricia Poorthunder; Sandra Sangster;
Nancy Scurlock, MSN, ANP-C, CDE; Leigh A. Shovestul , RD,
University of Pittsburgh. David E. Kel ey, MD (Principal
CDE; Janelia Smiley; Katie Toledo, MS, LPC; Christina Tom-
Investigator); Jacqueline Wesche-Thobaben, RN, BSN, CDE chee, BA; Darryl Tonemah PhD.
(Program Coordinator); Lewis Kul er, MD, DrPH (Co-investi-
gator); Andrea Kriska, PhD (Co-investigator); Janet Bonk, RN, University of Southern California. Anne Peters, MD (Prin-
MPH; Rebecca Danchenko, BS; Daniel Edmundowicz, MD cipal Investigator); Valerie Ruelas, MSW, LCSW (Program
articles intervention and Prevention
Co ordinator); Siran Ghazarian Sengardi, MD (Program Coordi-
046204); and the Frederic C. Bartter General Clinical Research Center
nator); Kathryn Graves, MPH, RD, CDE; Kati Konersman, MA, (grant M01RR01346). The following organizations have committed to make
RD, CDE; Sara Serafin-Dokhan. Coordinating Center.
major contributions to Look AHEAD: Federal Express; Health Management Resources; Johnson & Johnson, LifeScan Inc.; Optifast-Novartis Nutrition; Roche Pharmaceuticals; Ross Product Division of Abbott Laboratories;
Wake Forest University. Mark A. Espeland, PhD (Principal
Slim-Fast Foods Company; and Unilever. Additional support was received
Investigator); Judy L. Bahnson, BA (Program Coordinator); from K23HL109235 (L.F.F.).
Lynne Wagenknecht, DrPH (Co-investigator); David Rebous-
sin, PhD (Co-investigator); W. Jack Rejeski, PhD (Co-investi-
dIsclosure The authors declared no conflict of interest.
gator); Alain Bertoni, MD, MPH (Co-investigator); Wei Lang,
PhD (Co-investigator); Gary Miller, PhD (Co-investigator); 2011 The Obesity Society
David Lefkowitz, MD (Co-investigator); Patrick S. Reynolds,
MD (Co-investigator); Paul Ribisl, PhD (Co-investigator); reFerences
1. Keys A. Biology of Human Starvation. Minneapolis: University of Minnesota
Mara Vitolins, DrPH (Co-investigator); Michael Booth, MBA
(Program Coordinator); Kathy M. Dotson, BA (Program Coor-
2. Stunkard AJ. The dieting depression; incidence and clinical characteristics of
dinator); Amelia Hodges, BS (Program Coordinator); Carrie
untoward responses to weight reduction regimens. Am J Med 1957;23: 77–86.
C. Williams, BS (Program Coordinator); Jerry M. Barnes, MA; 3. Chaput JP, Arguin H, Gagnon C, Tremblay A. Increase in depression
Patricia A. Feeney, MS; Jason Griffin, BS; Lea Harvin, BS; Wil-
symptoms with weight loss: association with glucose homeostasis and
liam Herman, MD, MPH; Patricia Hogan, MS; Sarah Jaramillo,
thyroid function. Appl Physiol Nutr Metab 2008;33:86–92.
MS; Mark King, BS; Kathy Lane, BS; Rebecca Neiberg, MS; 4. Pagoto S, Bodenlos JS, Kantor L et al. Association of major depression and
binge eating disorder with weight loss in a clinical setting. Obesity (Silver
Andrea Ruggiero, MS; Christian Speas, BS; Michael P. Walkup,
MS; Karen Wall, AAS; Michelle Ward; Delia S. West, PhD; 5. Ludman E, Simon GE, Ichikawa LE et al. Does depression reduce the
effectiveness of behavioral weight loss treatment? Behav Med 2010;35: 126–134.
6. McFarlane T, Polivy J, McCale RE. Help, not harm: psychological foundation
Federal sponsors
for a nondieting approach toward health. J Soc Issues 1999;55:261–276. National Institute of Diabetes and Digestive and Kidney Diseases.
7. Campos P. The Obesity Myth: Why America’s Obsession with Weight is Hazardous to Your Health. New York: Gotham Books; 2005.
Barbara Harrison, MS; Van S. Hubbard, MD PhD; Susan 8. Brinkworth GD, Buckley JD, Noakes M, Clifton PM, Wilson CJ. Long-term
Z.Yanovski, MD. National Heart, Lung, and Blood Institute:
effects of a very low-carbohydrate diet and a low-fat diet on mood and
Lawton S. Cooper, MD, MPH; Jeffrey Cutler, MD, MPH; Eva
cognitive function. Arch Intern Med 2009;169:1873–1880.
9. Hainer V, Hlavatá K, Gojová M et al. Hormonal and psychobehavioral
predictors of weight loss in response to a short-term weight reduction program in obese women. Physiol Res 2008;57 Suppl 1:S17–S27. Centers for Disease Control and Prevention. Edward W. Gregg,
10. Wadden TA, Foster GD, Letizia KA. One-year behavioral treatment of
PhD; David F. Williamson, PhD; Ping Zhang, PhD.
obesity: comparison of moderate and severe caloric restriction and the effects of weight maintenance therapy. J Consult Clin Psychol 1994;62: 165–171. acknowledGMents
11. Rubin RR, Knowler WC, Ma Y et al.; Diabetes Prevention Program
Michael Walkup, M.S. had full access to all of the data in the study and
Research Group. Depression symptoms and antidepressant medicine
takes responsibility for the integrity of the data and the accuracy of the data
use in Diabetes Prevention Program participants. Diabetes Care
analysis. This study was supported by the Department of Health and Human
Services through the following cooperative agreements from the National
12. Clark MM, Niaura R, King TK, Pera V. Depression, smoking, activity level,
Institutes of Health: DK57136, DK57149, DK56990, DK57177, DK57171,
and health status: pretreatment predictors of attrition in obesity treatment.
DK57151, DK57182, DK57131, DK57002, DK57078, DK57154, DK57178,
Addict Behav 1996;21:509–513.
DK57219, DK57008, DK57135, and DK56992. The following federal
13. Marcus MD, Wing RR, Guare J, Blair EH, Jawad A. Lifetime prevalence
agencies have contributed support: National Institute of Diabetes and
of major depression and its effect on treatment outcome in obese type II
Digestive and Kidney Diseases; National Heart, Lung, and Blood Institute;
diabetic patients. Diabetes Care 1992;15:253–255.
National Institute of Nursing Research; National Center on Minority Health
14. Faulconbridge LF, Wadden TA, Berkowitz RI et al. Changes in symptoms
and Health Disparities; Office of Research on Women’s Health; Centers for
of depression with weight loss: results of a randomized trial. Obesity (Silver
Disease Control and Prevention; and the Department of Veterans Affairs.
This research was supported in part by the Intramural Research Program
15. Linde JA, Jeffery RW, Levy RL et al. Binge eating disorder, weight control
of the National Institute of Diabetes and Digestive and Kidney Diseases.
self-efficacy, and depression in overweight men and women. Int J Obes Relat Metab Disord 2004;28:418–425.
The Indian Health Service provided personnel, medical oversight, and
16. Jeffery RW, Sherwood NE, Brelje K et al. Mail and phone interventions for
use of facilities. Additional support was received from The Johns Hopkins
weight loss in a managed-care setting: Weigh-To-Be one-year outcomes. Int
Medical Institutions Bayview General Clinical Research Center (grant
J Obes Relat Metab Disord 2003;27:1584–1592.
M01RR02719); the Massachusetts General Hospital Mallinckrodt General
17. Delahanty LM, Meigs JB, Hayden D, Williamson DA, Nathan DM; Diabetes
Clinical Research Center and the Massachusetts Institute of Technology
Prevenion Program (DPP) Research Group. Psychological and behavioral
General Clinical Research Center (grant M01RR01066); the University of
correlates of baseline BMI in the diabetes prevention program (DPP).
Colorado Health Sciences Center General Clinical Research Center (grant
Diabetes Care 2002;25:1992–1998.
M01RR00051) and Clinical Nutrition Research Unit (grant P30 DK48520);
18. Finer N, James WP, Kopelman PG, Lean ME, Williams G. One-year
the University of Tennessee at Memphis General Clinical Research Center
treatment of obesity: a randomized, double-blind, placebo-controlled,
(grant M01RR0021140); the University of Pittsburgh General Clinical
multicentre study of orlistat, a gastrointestinal lipase inhibitor. Int J Obes
Research Center (grant M01RR000056) and the Clinical Translational
Relat Metab Disord 2000;24:306–313.
Research Center funded by the Clinical and Translational Science Award
19. Tate DF, Wing RR, Winett RA. Using Internet technology to deliver a
(grant UL1 RR 024153) and National Institutes of Health grant (grant DK
behavioral weight loss program. JAMA 2001;285:1172–1177. www.obesityjournal.org articles intervention and Prevention
20. Tsai AG, Wadden TA, Sarwer DB et al. Metabolic syndrome and health-
31. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for
related quality of life in obese individuals seeking weight reduction. Obesity
measuring depression. Arch Gen Psychiatry 1961;4:561–571. (Silver Spring) 2008;16:59–63.
32. Lustman PJ, Clouse RE, Griffith LS, Carney RM, Freedland KE. Screening
21. Wadden TA, Berkowitz RI, Sarwer DB, Prus-Wisniewski R, Steinberg C.
for depression in diabetes using the Beck Depression Inventory. Psychosom
Benefits of lifestyle modification in the pharmacologic treatment of obesity: a
randomized trial. Arch Intern Med 2001;161:218–227.
33. Beck AT, Steer, RA. Beck Depression Inventory Manual. In: Corporation TP
22. Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalence of
(ed.) San Antonio: Harcourt Brace & Company; 1987.
comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care
34. Spitzer RL, Yanovski S, Marcus MD. Binge Eating Disorder Clinical Interview.
Pittsburgh, PA: Behavioral Measurement Database Services; 1994.
23. Egede LE, Zheng D. Independent factors associated with major depressive
35. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health
disorder in a national sample of individuals with diabetes. Diabetes Care
survey (SF-36). I. Conceptual framework and item selection. Med Care
24. Look AHEAD Research Group, Pi-Sunyer X, Blackburn G et al. Reduction
36. Tang TZ, DeRubeis RJ. Sudden gains and critical sessions in cognitive-
in weight and cardiovascular disease risk factors in individuals with type
behavioral therapy for depression. J Consult Clin Psychol 1999;67:
2 diabetes: one-year results of the look AHEAD trial. Diabetes Care
37. Rubin RR, Ma Y, Marrero DG et al.; Diabetes Prevention Program Research
25. Williamson DA, Rejeski J, Lang W et al.; Look AHEAD Research Group.
Group. Elevated depression symptoms, antidepressant medicine use,
Impact of a weight management program on health-related quality
and risk of developing diabetes during the diabetes prevention program.
of life in overweight adults with type 2 diabetes. Arch Intern MedDiabetes Care 2008;31:420–426.
38. Wadden TA, Berkowitz RI, Womble LG et al. Randomized trial of
26. US Food and Drug Administration Advisory Committee. FDA Briefing
lifestyle modification and pharmacotherapy for obesity. N Engl J Med
Document: Zimulti (rimonabant) Tablets, 20 mg. Rockville: FSA; Assessed
39. Wirth A, Krause J. Long-term weight loss with sibutramine: a randomized
27. Christensen R, Kristensen PK, Bartels EM, Bliddal H, Astrup A. Efficacy and
controlled trial. JAMA 2001;286:1331–1339.
safety of the weight-loss drug rimonabant: a meta-analysis of randomised
40. Gorin AA, Niemeier HM, Hogan P et al.; Look AHEAD Research Group.
trials. Lancet 2007;370:1706–1713.
Binge eating and weight loss outcomes in overweight and obese individuals
28. Ryan DH, Espeland MA, Foster GD et al.; Look AHEAD Research Group.
with type 2 diabetes: results from the Look AHEAD trial. Arch Gen Psychiatry
Look AHEAD (Action for Health in Diabetes): design and methods for a
clinical trial of weight loss for the prevention of cardiovascular disease in type
41. Department of Health and Human Service, Public Health Service, Food
2 diabetes. Control Clin Trials 2003;24:610–628.
and Drug Administration Center for Drug Evaluation and Research
29. Wadden TA, West DS, Neiberg RH et al.; Look AHEAD Research Group.
Memorandum, 16 November 2006: Overview for December 13 Meeting
One-year weight losses in the Look AHEAD study: factors associated with
of Psychopharmacologic Drugs Advisory Committee (PDAC). Appendix 2:
success. Obesity (Silver Spring) 2009;17:713–722.
Request to Sponsors - Advice for the pharmaceutical industry in exploring
30. Diabetes Prevention Program (DPP) Research Group. The Diabetes
their placebo-controlled clinical trials databases for suicidality and preparing
Prevention Program (DPP): description of lifestyle intervention. Diabetes Care
data sets for analysis by FDA. <http://www.fda.gov/ohrms/dockets/ac/06/
List of Growers/Beneficiaries under Technology Mission for the year 2012-13 Biodata of Beneficiaries District Constituency Particulars of activity Amount paid Remarks if any Activity Gh.Hassan Dar S/o Late Qasim Dar R/o Dub Ganderbal Master Gh.Mohd Bhat S/o Late Mohd Sultan Bhat R/o Masooda Yasmin S/o Late Ahmadullah Gillani R/o Kharbagh
Informationen zur Neuen Grippe (Influenza A/H1N1) für Schulleitungen 1. Situationseinschätzung Deutschland Das Virus A/H1N1, das die Neue Grippe verursacht, kann leicht von Mensch zu Mensch übertragen werden. Das zeigt die ständig steigende Zahl der Erkrankten. Derzeit sind in Deutschland 16.835 Personen an der Neu-en Grippe erkrankt (Stand 04. September 2009). Die Mehrzahl d
 articles
articles