Braz Dent J (2007) 18(3): 244-247 Importance of the Diagnosis in the Pulpotomy of Immature Permanent Teeth 1School of Dentistry, University of Ribeirão Preto, Ribeirão Preto, SP, Brazil2School of Dentistry, Bahia State Foundation for Science Development, Salvador, BA, Brazil3School of Dentistry of Ribeirão Preto, University of São Paulo, Ribeirão Preto, SP, Brazil
Pulpotomy is a conservative therapy performed to remove the inflamed coronal portion of the pulp and preserve the vitality of theremaining radicular pulp. This article reports two cases of immature permanent mandibular molars with clinical signs of pulp vitalityand radiographic images of periapical bone rarefaction, which were treated with calcium hydroxide pulpotomy. In Case 1, pulpotomywas performed in a single session, while in Case 2 two sessions were required to complete the treatment. Clinical and radiographicfollow up within 13 and 9 months, respectively, showed hard tissue barrier and new bone formation as well as progression of rootdevelopment. These outcomes are confirmatory that an accurate clinical/radiographic assessment of pulp vitality is of paramountimportance for the correct diagnosis and indication of pulpotomy in cases of young permanent teeth with incomplete root formation.
Key Words: pulpotomy, diagnosis, calcium hydroxide, periapical lesion. INTRODUCTION
should aim at its complete repair and formation of amineralized barrier that covers the exposed area com-
The dental pulp is an innervated and vascularized
tissue that is able to react to physical, chemical and
Pulpotomy comprises coronal pulp amputation
biological stimuli and promote an adequate healing, with
and placement of a protective agent over the remaining
formation of a hard tissue barrier (1). If the stimulus or
viable root pulp in order to preserve its vitality and
damage is severe, the pulp healing capacity may be
function (2,3). It is indicated for primary or young
exceeded and it may progress to an irreversibly inflamed
permanent teeth with inflamed and/or infected coronal
condition and to necrosis. However, if pulp exposure is
pulp. However, the presence of periapical rarefaction
discrete in primary or young permanent teeth, some
has been presented as a condition that contraindicates
procedures may be performed in an attempt to reestablish
pulpal health and maintain its vitality (1-3).
By presenting two cases of immature permanent
Pulp exposure is defined in the MeSH (Index
mandibular molars with radiographic image of periapi-
Medicus: Medical Subject Headings) as “the result of
cal lesion submitted to calcium hydroxide pulpotomy,
pathological changes in the hard tissue of a tooth caused
the purpose of this article is to discuss, based on the
by carious lesions, mechanical factors or trauma, which
treatment outcomes and on the literature, whether
render the pulp susceptible to bacterial invasion from the
periapical bone rarefaction is actually a contraindication
external environment”. The treatment of pulp exposure
Correspondence: Prof. Ronaldo Araújo Souza, Avenida Paulo VI, 2038/504, Ed. Villa Marta, 41810-001 Salvador, BA, Brasil. Tel/Fax:+55-71-3358-5396. e-mail: [email protected]Diagnosis and pulpotomy of immature permanent teethCASE REPORT
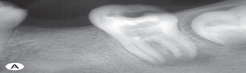
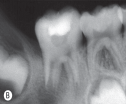
face due to the drainage of an extraoral fistula. Thepreoperative radiograph showed a furcation lesion com-
municating with the a periapical lesion associated with
A 7-year-old female patient was referred for
the distal root of that tooth (Fig 2A). After anesthesia,
treatment of the mandibular left first molar that pre-
rubber dam placement and carious tissue excavation,
sented a deep caries and radiographic image suggestive
access to pulp chamber was gained. A vital pulp tissue
of periapical lesion (Fig. 1A). Pulp vitality test was not
was observed with normal consistence and bleeding
performed because of the clinical aspect of the carious
lesion associated with the well-defined image of periapi-
As the patient was uncooperative, pulpotomy
was scheduled as two-session procedure. In the first
After anesthesia, rubber dam placement and
session, the coronal pulp was partially excised with
carious tissue excavation, access to pulp chamber was
sharp curettes under copious irrigation with calcium
gained. A vital pulp tissue was observed with normal
hydroxide solution alternated with aspiration. After
consistence and bleeding characteristics. The coronal
hemostasis, the remaining coronal pulp tissue was dried
pulp was excised with sharp curettes under copious
pressureless with sterile cotton pellets and protected
irrigation with calcium hydroxide solution alternated
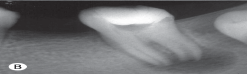
with a calcium hydroxide/saline paste. The pulp cham-
with aspiration. After hemostasis, the area of the ex-
ber was provisionally sealed with the quick-setting zinc
posed root pulp tissue was dried pressureless with
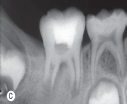
oxide and eugenol-based cement (Fig. 2B).
sterile cotton pellets and the pulp chamber floor was
At the second session, the patient was anesthe-
capped with a calcium hydroxide/saline paste, sealing
tized, a rubber dam was placed, the provisional restora-
root canal entrances. A sterile cotton mesh was placed
tion was removed and pulpotomy was completed in the
over the paste and the pulp chamber was sealed with a
same way as performed in the first session. The distal
quick-setting zinc oxide and eugenol-based cement
root canal presented darkened bleeding and the pulp
tissue was less resistant to cutting with the curettes.
The periapical radiographs taken 13 months after
Thus, pulp amputation proceeded 2 mm beyond the
pulpotomy revealed complete regression of the periapical
canal entrance, at which point normal live red bleeding
lesion with periradicular bone tissue formation, normal
and resistance to cutting were observed.
root development and recovery of the apical periodontal
After hemostasis, the area of the exposed root
ligament space and lamina dura (Figs. 1B and 1C).
pulp tissue was dried pressureless with sterile cottonpellets and the pulp chamber floor was covered with a
calcium hydroxide/saline paste, sealing root canal en-
A 6-year-old male patient was referred by the
trances. A sterile cotton mesh was placed over the paste
periodontist with a dressing on the lower right side of the
and the pulp chamber was sealed with the quick setting
Figure 1. Radiographic follow-up of a pulpotomized immature permanent mandibular left first molar with vital pulp. (A) Preoperativeperiapical radiograph showing periapical bone rarefaction. (B) Radiographic aspect after calcium hydroxide pulpotomy. (C) Thirteen-month control radiograph, showing resolution of the periapical lesion, normal root development, recovery of the apical periodontalligament space and lamina dura on both roots.
zinc oxide and eugenol-based cement (Fig. 2C).
response to persist and extend to a more apical portion
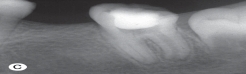
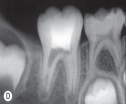
The periapical radiographs taken 9 months after
of the pulp tissue. This process is repeated successively
pulpotomy revealed complete regression of the periapi-
until the entire pulp tissue is affected (5).
cal and furcation lesions, formation of a hard tissue
In some cases, especially in immature teeth,
barrier and normal root development (Fig. 2D).
before pulp necrosis is completed, chemical mediatorsof bone resorption, enzymes and products from protein
DISCUSSION
decomposition may cross the remaining healthy pulptissue and cause periradicular alterations (6). Thus, in
Caries progression and pulp exposure permit
spite of their vitality, these teeth develop periapical
microbial invasion into the pulp chamber and vascular
lesions, as shown in both cases reported in this article.
and tissue alterations become strongly evident. The
Therefore, a correct diagnosis is of paramount
severity of the inflammatory response increases pro-
importance for institution of the most indicated treat-
gressively, leading to pulp necrosis and formation of
ment modality. Clinical examination, comprising caries
micro-abscesses. Pulp alterations are, however, local
excavation and observation of sensitivity on tissue
events (5). As the inflammatory reaction becomes
removal, palpation of vestibules and pulp vitality tests
stronger, a greater amount of chemical mediators and
should preceede the radiographic examination in the
enzymes is released, which causes the inflammatory
Figure 2. Radiographic follow-up of a pulpotomized immature permanent mandibular right first molar with vital pulp. (A) Preoperativeperiapical radiograph showing furcation lesion communicating with a periapical lesion on the distal root. (B and C) Radiographic aspectafter calcium hydroxide pulpotomy (note that the deeper level of pulp amputation in the distal root). (D) Nine-month controlradiograph, showing resolution of the furcation and periapical lesion and normal root development. Diagnosis and pulpotomy of immature permanent teeth
Several materials have been used as pulp-capping
pela técnica da pulpotomia com hidróxido de cálcio. No caso 1 a
agents in pulpotomized teeth, among which formocresol,
pulpotomia foi realizada em sessão única e no caso 2 em duassessões. A proservação clínica e radiográfica com 13 e 9 meses,
calcium hydroxide, ferrous sulfate and more recently
respectivamente, evidenciou formação de barreira mineralizada,
mineral trioxide aggregate (1,3,4,7,8). Some of these
neoformação óssea e desenvolvimento radicular. Conclui-se que a
materials, like calcium hydroxide, are able to induce the
avaliação clínica da vitalidade pulpar, complementada pela análise
formation of a hard-tissue tissue barrier (1,3,8). In
radiográfica, é fundamental para o correto diagnóstico e indicaçãode pulpotomia em casos de dentes permanentes jovens com
addition to this property, calcium hydroxide is also
capable of stimulating pulp tissue repair and presents thebest pulp capping outcomes (1,8-12). REFERENCES
When calcium hydroxide is placed in direct
contact with the pulp tissue, there is an immediate and
1. Albuquerque DS, Gominho LF, Santos RA. Histologic evalua-
short-term tissue reaction supposedly caused by its high
tion of pulpotomy performed with ethyl-cyanoacrylate andcalcium hydroxide. Braz Oral Res 2006;20:226-230.
alkalinity. This alkaline effect is due to the release of
2. Markovic D, Zivojinovic V, Vucetic M. Evaluation of three
hydroxyl ions, which, in contact with the vital tissue,
pulpotomy medicaments in primary teeth. Eur J Paediatr
produce morphological changes that are histologically
3. Huth KC, Paschos E, Hajek-Al-Khatar N, Hollweck R, Crispin
characterized by the presence of self-limiting superficial
A, Hickel R, Folwaczny M. Effectiveness of 4 pulpotomy
necrosis in their early stage (13). Moreover, it has been
techniques-randomized controlled trial. J Dent Res
reported (14) that the alkaline environment avoids bac-
4. Olsson H, Petersson K, Rohlin M. Formation of a hard tissue
terial proliferation, which is of paramount importance
barrier after pulp capping in humans. A systematic review. Int
because tissue repair and mineralized tissue deposition
only occur in the absence of an infectious process.
5. Ricucci D. Apical limit of root canal instrumentation and
obturation, part 1. Literature review. Int Endod J
In vivo studies (1,8) have demonstrated that
calcium hydroxide is an excellent choice for cases of
6. Langeland K. Management of the inflamed pulp associated
pulpotomy, present high rates of hard tissue barrier
with deep carious lesion. J Endodon 1981;7:169-181.
formation and sealing of pulp exposure, maintaining the
7. Cengiz SB, Batirbaygil Y, Onur MA, Atilla P, Asan E, Altay N,
Cehreli ZC. Histological comparison of alendronate, calcium
integrity and vitality of the remaining root pulp. Accord-
hydroxide and formocresol in amputated rat molar. Dental
ingly, in both cases reported in this article, hard-tissue
barrier and periapical new bone formation was observed
8. Tunç ES, Saroglu I, Sari S, Günhan Ö. The effect of sodium
hypochlorite application on the success of calcium hydroxide
in addition to normal root development.
pulpotomy in primary teeth. Oral Surg Oral Med Oral Pathol
In view of this, it may be concluded that the
diagnosis of pulp and/or periradicular alterations in
9. Trope M, McDougal R, Levin L, May KN, Swift EJ. Capping
the inflamed pulp under different clinical conditions. J Esthet
immature permanent teeth should not rely exclusively
on radiographic findings. A detailed clinical examination,
10. Hörsted-Bindslev P, Vilkinis V, Sidlauskas A. Direct capping of
comprising pulp vitality, percussion and palpation tests,
human pulps with a dentin bonding system or with calcium
should be complemented by the evaluation of character-
hydroxide. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2003;96:591-600.
istics such as pulp firmness (resistance to cutting with
11. Conrado CA. Remineralization of carious dentin. I: In vitro
curettes), color and type of bleeding. With proper case
microradiographic study in human teeth capped by calcium
selection and indication, calcium hydroxide pulpotomy
hydroxide. Braz Dent J 2004;15:59-62.
12. Briso AL, Rahal V, Mestrener SR, Dezan Junior E. Biological
may be a feasible and valuable treatment modality for
response of pulps submitted to different capping materials.
immature permanent teeth, even those associated with
a radiographic image suggestive of periapical lesion.
13. Schröder U. Effects of calcium hydroxide-containing pulp-
capping agents on pulp cell migration, proliferation, anddifferentiation. J Dent Res 1985;64:541-548.
14. Cvek M. Treatment of non-vital permanent incisors with
calcium hydroxide. Odont Rev 1972;23:27-44.
A pulpotomia é uma terapia conservadora indicada para dentes
15. Caliskan MK. Pulpotomy of carious vital teeth with periapical
involvement. Int Endod J 1995;28:172-176.
vitais com alterações inflamatórias da polpa dental coronária. Esse artigo relata dois casos de molares inferiores com rizogêneseincompleta e imagem radiográfica de rarefação periapical que,
clinicamente, apresentavam vitalidade pulpar e foram tratados
DRUGS – die Partydrogeninfo! Alles was du schon immer über Partydrogen wissen wolltest und noch nie ehrlich beantwortet wurde . Dieser Text umfasst die vollständige Fassung der Broschüre „DRUGS – die Partdrogeninfo!“ in d e r F a s s u n g der 4. völlig neu bearbeiteten und erweiterten Auflage vom Sommer 2001 mit den Ergänzungen des „Updates“ vom Sommer 2003.
Bayer Environmental Science Material Safety Data Sheet Bayer Advance Garden® Ant and Wasp Dust Ready-to-use Puffer SECTION 1: IDENTIFICATION OF THE MATERIAL AND SUPPLIER Bayer Advanced Garden® Ant and Wasp Dust Ready-to- use Puffer A Business Operation of Bayer CropScience Pty Ltd ABN 87 000 226 022 391-393 Tooronga Road, East Hawthorn Victoria 3123, Australia Technical Informat
 Diagnosis and pulpotomy of immature permanent teeth
CASE REPORT
Diagnosis and pulpotomy of immature permanent teeth
CASE REPORT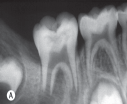
 zinc oxide and eugenol-based cement (Fig. 2C).
zinc oxide and eugenol-based cement (Fig. 2C).