Addictive Behaviors xx (2006) xxx – xxx
Long term success of short smoking cessation seminars
Department of Preventive Medicine, Institute of Environmental Health, Medical University of Vienna,
Kinderspitalgasse 15, A-1095 Wien, Austria
The objective of this longitudinal (3 year) study was to determine predictors of abstinence in 515 employees of a
steel plant (28% female, age 18–67 years) after participation in Allen Carr seminars (intensive group counselling in asingle session of 6 h). Answers given in computer aided phone interviews were analysed by stepwise and Coxregression. Of 510 responding persons 262 (51.4%) reported continuing abstinence. In a random sample of 61respondents cotinine concentration in urine was measured, showing high agreement with smoking history. Socialsupport increased abstinence, which was more persistent in males and office workers. Also in female participants thenon-smoking spouse was a significant predictor for abstinence while a higher body weight predicted relapse. Relapsed female smokers did not show a sustainable reduction of cigarette consumption. Compared to cessationclinics higher population coverage would be achievable by workplace seminars. Every second smoker motivated toparticipate seems to be able to quit even without medication and to stay abstinent. Especially in females theseseminars should be followed by physical exercise and continued support of gender specific occupational health care. 2006 Elsevier Ltd. All rights reserved.
Keywords: Smoking cessation; Workplace; Group counselling; Occupational health; Cotinine
Since cessation rates in the general population have been reported to increase with the introduction of
smoke-free workplaces (many countries added workplace interventions to the priorities of tobacco control. Appropriate legislationwas still missing when this study was performed in the largest steel company of Austria, which has a long
0306-4603/$ - see front matter 2006 Elsevier Ltd. All rights reserved. doi:
Please cite this article as: H. Moshammer, M. Neuberger, Long term success of short smoking cessation seminars supported by occupationalhealth care, Addictive Behaviors (2006),
H. Moshammer, M. Neuberger / Addictive Behaviors xx (2006) xxx–xxx
tradition of preventive occupational medicine and decided already in 1999 to offer free seminars forsmoking cessation to its workforce, using the services of Easyway® and the method of . The aim of this study was to analyse the determinants for successful quitting ) over a longer period of time and in a less heterogeneous occupational setting than the only studyhaving evaluated such seminars before (), which are used forsmoking cessation at the workplace in many European countries.
Recent reviews concluded that there is not enough evidence yet to know whether group therapy is as
effective as individual therapy and that workplace programs for smokingcessation increase cessation in persons already motivated ) and reduce the number of cigarettes smoked during the workday only, with conflicting evidenceabout whether they reduce overall cigarette consumption by smokers (). These conclusions seem to be based on studies mainly focused on pharmacotherapy. Both populationstudies and clinical trials () usingpharmacotherapy reported 1-year abstinence rates around 15% only. In one study the combination ofnicotine and bupropion reached success rates of 35.5% compared to placebo (), butwith counselling sessions of 15 min or less the motivational part did not seem to be of primary importanceand was not evaluated separately.
The method of intervention (intensive group counselling in a single session of 6 h) has been described
previously ): The trainer tells the participants to keep smoking while they listen to himso they can analyse why they do it. He makes the smoker discover that most cigarettes he is not smokingfor enjoyment but because of addiction. Instead of going “cold turkey” and feeling deprived, the smokershould feel that he is doing something positive and looking forward to a great life. A significant andsustainable improvement of subjective life quality after the seminar has been proven. Such seminars wereorganised by a large Austrian steel company. They were open for everybody but mostly advertised withinthe company which allowed their employees to attend the seminars during working time. From November1999 to December 2001 a total of 1311 persons participated, including spouses, other family membersand partners of employees. Only afterwards it was decided to evaluate the success of the seminars, butonly the names of the participants were available then. From these participation lists persons were soughtin chronological order in the telephone directory of the steel factory. When 792 participants had beenchecked 686 of them were found in the directory and of these 171 (25%) were not reached in 4 attempts. Of 515 contacted between December 2003 and November 2004 five persons (1%) refused an answer(despite of confirmation that all personal data would be stored at the university only and destroyed aftercalculations to guarantee anonymity). gives the basic characteristics of the study group beforeintervention as reported by the 510 persons retrospectively. While all respondents answered the questionsregarding current smoking behaviour, the full set of answers was only provided by 483 participants. Sonot all statistics are based on exactly the same number of subjects.
The computer aided phone interviews were based on a standardised form including questions
concerning previous and current smoking behaviour and personal factors as detailed below. The answerswere analysed for duration of abstinence after the seminar by Cox regression, using SPSS 11.5. Multiplestepwise regression analysed four groups of determinants: a) smoking behaviour before the seminar:
Please cite this article as: H. Moshammer, M. Neuberger, Long term success of short smoking cessation seminars supported by occupationalhealth care, Addictive Behaviors (2006), doi:
H. Moshammer, M. Neuberger / Addictive Behaviors xx (2006) xxx–xxx
Table 1Description of subjects (n = 510) prior to intervention for the whole group and by outcome
number of daily cigarettes and years smoking; b) personal and socio-economic: sex, age, blue (manual)/white collar (office) worker, shift work; c) weight and subjective health before the seminar (general statusof health and susceptibility to infections). The latter two were presented in 5 categories each; theresponses were treated as equally distributed nominal variables. The effect estimates are presented as perone unit change; d) psychosocial: number of work-mates in seminar, smoking status of spouse/partner,strength of own wish to stop smoking, smoking ban at the workplace. (At the time of the study smokingwas not banned because of protection of non-smokers, but only at few workplaces because of fire hazard). Each group of determinants (a–d) was analysed separately: Originally all determinants of each groupwere entered into the model but then starting with the least influential variable (highest p-value) allvariables with p N 0.2 were excluded stepwise.
For biochemical validation of results the following procedure was agreed with the workers' council:
From routine preventive screening examinations of all workers after the telephone survey (offered as afree health screening including electrocardiogram, blood and urine tests without connection to theprevious seminar) parts of urine samples were used until 30 participants with a history of continuing non-smoking and 30 participants with a history of relapse to smoking had been tested for excretion of cotinine. This way urine samples of 61 persons were collected, cotinine concentrations were analysed and related todaily number of cigarettes smoked. Kappa values as measure of agreement between smoking history andurinary cotinine were calculated.
In random samples of 30 smokers and 31 non-smokers according to history the agreement with results
from urinary cotinine concentrations was high: The Kappa was 0.9 with a cut-off at 600 ng/ml. Reportednumber of cigarettes was correlated significantly with urinary cotinine concentrations (r = 0.84). Urinarycotinine concentrations in 5 persons reporting relapse to smoking were found to be below 600 ng/ml,while in 5 persons reporting continuing abstinence they were found above this cut-off. Repeated tests ofthe latter revealed occasional smoking in one case and non-smoking confirmed by cotinine concentrationsbelow 600 ng/ml in 4 cases. In the biochemical validation it is important to remember that both relapsersand abstinence maintainers exposed to environmental tobacco smoke (ETS) can present higher cotinineconcentrations than expected (Tests for cotinine used to validate
Please cite this article as: H. Moshammer, M. Neuberger, Long term success of short smoking cessation seminars supported by occupationalhealth care, Addictive Behaviors (2006),
H. Moshammer, M. Neuberger / Addictive Behaviors xx (2006) xxx–xxx
smoking histories have been reported to achieve a sensitivity of 96–97% and specificity of 99–100%).
At interviews conducted 2–4 1/2 years (mean 3 years) after the seminar no participant reported use of
bupropion and 10 of the 12 participants who used nicotine replacement therapy (NRT) had a relapse tosmoking. Of the 27 participants who answered only to the question on smoking status 13 reported continuingnon-smoking (48.1%). Of the remaining 483 persons (348 males, 135 females) who gave a complete interview,249 (51.6%) reported continuing non-smoking and 234 (48.4%) reported relapse to smoking. Assuming all 5persons who did not answer to be smokers, the total relapse rate was 49.1%. Most relapses occurred shortlyafter the seminar; only a single person reported relapse after more than two years of abstinence.
Selected determinants for long term success of the seminar are shown in and . Smoking
behaviour before the seminar did not influence cessation. In the total group social support was found mostimportant. Long term success was significantly better if more work-mates from the same departmentparticipated in the seminar and if the spouse/partner did not smoke. Relapse was more frequent in bluecollar workers, but even in this group stayed below 60%. Males stayed abstinent more often than females,and relapsed male smokers had reduced their cigarette consumption more (−3.8 cigarettes/day onaverage) than relapsed female smokers (−2.6). Successful participants reported more frequently about apoor status of health before the seminar. This was not seen when females were analysed separately( p = 0.918): In contrast to the general results which are dominated by males, abstinence in females wasinfluenced by body weight before the seminar. With higher weight a trend to earlier relapse (RR = 1.021,p = 0.061) was seen. In females only the association with the smoking behaviour of the spouse/partnerreached statistical significance (RR = 2.77, p b 0.001).
Table 2Determinants of relapse to smoking (only variables with p b 0.2 remained in the final model)
Termination of abstinence (cox-regression)
Status of health before seminarBody weight
Psychosocial factorsSmoking ban at workplace
Please cite this article as: H. Moshammer, M. Neuberger, Long term success of short smoking cessation seminars supported by occupationalhealth care, Addictive Behaviors (2006), doi:
H. Moshammer, M. Neuberger / Addictive Behaviors xx (2006) xxx–xxx
Fig. 1. Kaplan–Meier plots of abstinence rate over 1500 days each: a) White collar workers (black) versus blue collar workers(grey); b) Non-smoking spouse / partner (black) versus smoking spouse / partner (grey); c) More than 6 participants at theseminars from the same work-place (black) versus 6 or less participants (grey); d) Poor health (3–5) before the seminar (black)versus good health (1 and 2, grey). Y-axis: percentage of non-smokers, X-axis: years.
At the time of the interview the relapsed persons reported a less favourable development of general
health and higher susceptibility to infection ( p b 0.001), both related to the number of cigarettes per day. While relapsed females kept their weight (on average a reduction of 0.94 kg was reported) the weight ofthe abstinent females increased by 4.4 kg.
Self selection of highly motivated persons has to be considered as a possible cause for unusually high
success rates, however, seminars at the workplace should suffer less from this selection bias than studies
Please cite this article as: H. Moshammer, M. Neuberger, Long term success of short smoking cessation seminars supported by occupationalhealth care, Addictive Behaviors (2006),
H. Moshammer, M. Neuberger / Addictive Behaviors xx (2006) xxx–xxx
on persons seeking medical aid, and they have the advantage of addressing smokers in early motivationalstages (who otherwise would not haveconsulted a doctor. Unfortunately it was not possible to interview a control group of workers who did notparticipate in a seminar. From routine representative health interviews in UpperAustria (where the enterprise is located) an annual quit rate of 3% was estimated (weighting by 5-year agegroups and sex). Routine histories of the occupational health department also showed that self-help quitrate was negligibly low in this enterprise before 2002 when implementation of the amendment of theworkers protection law started.
Selection bias cannot be excluded, but important selection of smokers highly motivated to quit seems
unlikely, because quit rates of participants in the first seminars offered at this company (assumed to be theones already motivated to quit) were not higher than of participants in later seminars. Some selection biasmight be due to accessibility by telephone, which could not be corrected according to , because of missing data. If age or shift work influenced accessibility by phone, bias wouldhave been negligible, because they had moderate to none effect on cessation (). Only in case thatblue collar workers were less accessible by phone than white collar workers some overestimation ofsuccess rates would have to be taken into account. A relevant influence of accessibility by sex is not likely.
Treating non-responders as smokers in smoking cessation research may underestimate the true effect of
cessation treatment ), but even making the conservativeassumption that all non-respondents had failed to abstain, the cessation rate after 3 (2–4.5) years was49.1% and after consideration of persons with incomplete answers and controlling for cotinine in additionit was 47%.
Questions of validity have been discussed for telephone interviews used for surveys of scattered populations
) and occupational cohorts Underreporting ) seems to be negligible compared to otherdifferences in cessation studies: Comparisons of smoking prevalence estimates derived from surveys usingtelephone versus in-person interviews have shown that the former are generally 1 to 3 percentage points belowthe latter. For adults, these concerns relate more to measures of the number of cigarettes smoked per day than tothe classification of whether a person is a current smoker
The determinants for successful quitting partly corroborate earlier results of Scandinavian studies on
smokers who had entered a cessation contest (list the following determinants as important: male sex, ageN40 years, living with a partner, low level of withdrawal symptoms, two or less previous quittingattempts, and support received from both health professionals and from lay persons (but not medication). We identified the non-smoking partner and the quitting work-mate as positive influences. If the colleaguescease tobacco consumption, then participants will have a reduced smoking setting, which can influencetheir own consumption ).
The results of the present study confirm that there is still a need to improve the seminars and aftercare with
regard to the special needs of women and to stress the importance of physical exercise during cessation. Ingeneral, however, the method successfully transmitted the positive feelings of a life after smoking cessation. In quitters general health scored by SF-36 improve (). After relapse at least the number ofcigarettes smoked was reduced significantly. Reduction of daily smoking was also related to smoking bans atthe workplace ). If smoking bans would protect the total workforce from passivesmoking, they could increase the cessation rate, too, and even motivate employees to stop smoking who didnot want to participate in the seminars up to now. In California smoke-free workplaces were associated with a
Please cite this article as: H. Moshammer, M. Neuberger, Long term success of short smoking cessation seminars supported by occupationalhealth care, Addictive Behaviors (2006), doi:
H. Moshammer, M. Neuberger / Addictive Behaviors xx (2006) xxx–xxx
reduction of total cigarette consumption of 29% due to 3.8% reduction in smoking prevalence and 3.1 fewercigarettes smoked per day per continuing smoker but in Austria tobaccolegislation still needs to be developed for achieving such goals.
The results of this study also support conclusions on effectiveness of methods from an Australian study
on general practice patients ) that smokers relying onpharmacological aid have much lower success rates than those quitting ‘cold turkey’. But since mostrelapses occurred during the first weeks and months supportive care should be intensified during thiscrucial period.
Our study in a large steel plant suggests that every second smoker motivated to quit smoking can
achieve permanent abstinence after only 6 h of professional counselling at his workplace, followed byoccupational health care and supported by work mates and family. Cessation seminars should be adaptedto special needs of women and blue collar workers. To enlarge the group of smokers willing to quit or toreduce their tobacco consumption improvements are needed in tobacco control legislation.
Both authors declare that they are and have been employed by a medical university, which will not gain
or lose financially from the results of this study. They acknowledge support in data collection from H. Csillag, A. Feuerstein, A. Herbst (occupational physicians of voestalpine, guarantor: H. Csillag) and agrant given by the Austrian Society for Occupational Medicine.
Burns, D. M., Shanks, T. G., Major, J. M., Gower, K. B., & Shopland, D. R. (2000). Restrictions on smoking in the workplace. In U.S.
Department of Health and Human Services, National Institutes of Health, & National Cancer Institute (Eds.), Population BasedSmoking Cessation. Monograph 12. NIH Publication, vol. 4892. (pp.) Bethesda, Maryland: National Institutes of Health.
Carr, A. (1991). The easy way to stop smoking. London: Penguin Books. Carr, A. (1998). How to stop your child smoking. Eastbourne, East Sussex: Gardners Books. Carr, A. (2002). Easy way for women to stop smoking. London: Arcturus Publishing. Doran, C. M. T., Lisa, V., Maxine, R., Helena, B., & Richard, P. M. (2006). Smoking status of Australian general practice
patients and their attempts to quit. Addictive Behaviors, 31, 758−766.
Ferguson, J., Bauld, L., Chesterman, J., & Judge, K. (2005). The English smoking treatment services: One-year outcomes.
Addiction, 100(Supplement 2), 59−69.
Fergusson, J. A., Patten, C. A., Schroeder, D. R., Offord, K. P., Eberman, K. M., & Hurt, R. D. (2003). Predictors of 6-month
tobacco abstinence among 1224 cigarette smokers treated for nicotine dependence. Addictive Behaviors, 28, 1203−1218.
Fichtenberg, C. M., & Glantz, S. A. (2002). Effect of smoke-free workplaces on smoking behaviour: Systematic review. British
Font-Mayolas, S., & Planes, M. (2000). Efectos del modelado por parte de familia, pareja y amigos en la conducta de fumar de
jsvenes universitarios [Role model effects of family, partners and friends on tobacco consumption in university students]. Adicciones, 12, 467−477.
Hutter, H. P., Moshammer, H., & Neuberger, M. (2006). Smoking cessation at the workplace: One year success of short
seminars. International Archives of Occupational and Environmental Health, 79, 42−48.
Jarvis, M. J., Tunstall-Pedoe, H., Feyerabend, C., Vesey, C., & Saloojee, Y. (1987). Comparison of tests used to distinguish
smokers from non-smokers. American Journal of Public Health, 77, 1435−1438.
Jorenby, D. E., Leischow, S. J., Nides, M. A., Rennard, S. I., Johnston, J. A., Hughes, A. R., et al. (1999). A controlled trial of
sustained-release bupropion, a nicotine patch, or both for smoking cessation. New England Journal of Medicine, 340,685−691.
Please cite this article as: H. Moshammer, M. Neuberger, Long term success of short smoking cessation seminars supported by occupationalhealth care, Addictive Behaviors (2006),
H. Moshammer, M. Neuberger / Addictive Behaviors xx (2006) xxx–xxx
Korhonen, T., Su, S., Korhonen, H. J., Uutela, A., & Puska, P. (1997). Evaluation of a national quit and win contest:
Determinants for successful quitting. Preventive Medicine, 26, 556−564.
Lancaster, T., & Stead, L. F. (2005). Individual behavioural counselling for smoking cessation. The cochrane database of
systematic reviews Oxford: Updated Software Issue 2, CD001292.
Li, Y. F., Langholz, B., Salam, M. T., & Gilliland, F. D. (2005). Maternal and grandmaternal smoking patterns are associated
with early childhood asthma. Chest, 127, 1232−1241.
Luepker, R. V., Pallonen, U. E., Murray, D. M., & Pirie, P. L. (1989). Validity of telephone surveys in assessing cigarette
smoking in young adults. American Journal of Public Health, 79, 202−204.
Moher, M., Hey, K., & Lancaster, T. (2005). Workplace interventions for smoking cessation. The cochrane database of
systematic reviews Oxford: Updated Software Issue 2, CD003440.
National Research Council (NRC, USA) (1986). Measuring exposures and assessing health effects. Environmental tobacco
smoke Washington, D.C.: National Academy Press.
Raber, A. (1983). Different selection rates — Fallacies in epidemiological studies. Zentralblatt für
Bakteriologie, Mikrobiologie und Hygiene, B, 177, 539−561.
Osinubi, O. Y., Moline, J., Rovner, E., Sinha, S., Perez-Lugo, M., Demissie, K., et al. (2003). A pilot study of telephone-based
smoking cessation intervention in asbestos workers. Journal of Occupational and Environmental Medicine, 45, 569−574.
Perez-Stable, E. J., Ramirez, A., Villareal, R., Talavera, G. A., Trapido, E., Suarez, L., et al. (2001). Cigarette smoking
behavior among US Latino men and women from different countries of origin. American Journal of Public Health, 91,1424−1430.
Pisinger, C., Vestbo, J., Borch-Johnsen, K., Thomsen, T., & Jorgensen, T. (2005). Acceptance of the smoking cessation
intervention in a large population-based study: The Inter99 study. Scandinavian Journal of Public Health, 33, 138−145.
Shaffer, H. J., Eber, G. B., Hall, M. N., & Bilt, J. V. (2000). Smoking behaviour among casino employees. Self-report validation
using plasma cotinine. Addictive Behaviors, 25, 693−704.
Smedslund, G., Fisher, K. J., Boles, S. M., & Lichtenstein, E. (2004). The effectiveness of workplace smoking cessation
programmes: A meta-analysis of recent studies. Tobacco Control, 13, 197−204.
Statistik Austria (2002). Rauchgewohnheiten: Ergebnisse des Mikrozensus Dezember 1997. Vienna, Austria: Statistik Austria.
Tillgren, P., Haglund, J. A., Ainetdin, T., & Holm, L. E. (1995). Who is a successful quitter? One-year follow-up of a national
quit and win contest in Sweden. Scandinavian Journal of Social Medicine, 23, 193−201.
Tomson, T., Bjornstrom, C., Gilljam, H., & Helgason, A. R. (2005). Are non-responders in a quitline evaluation more likely to
be smokers? BMC Public Health, 5, 52.
Please cite this article as: H. Moshammer, M. Neuberger, Long term success of short smoking cessation seminars supported by occupationalhealth care, Addictive Behaviors (2006), doi:
European Journal of Cancer 36 (2000) 1473±1478Recommendations on cancer screening in the European UnionAdvisory Committee on Cancer Prevention *Received 10 January 2000; accepted 22 February 2000excluding non-melanoma skin cancer, occurred in theEuropean Union in 1995. Of these, 2% were cervicalScreening allows the detection of cancers at an earlycancers, 13% breast cancers, 13% colorectal
In this study, we examine the distribution of revenues for a comprehensive sample of newdrugs introduced into the United States during the period, 1988 to 1992. In earlier research, weexamined the returns to R&D for the U.S. new drug introductions during the 1970s and early "The Distribution of Sales from Pharmaceutical Innovation" 1980s.[1,2] One of the key findings was that the

 Addictive Behaviors xx (2006) xxx – xxx
Long term success of short smoking cessation seminars
Department of Preventive Medicine, Institute of Environmental Health, Medical University of Vienna,
Kinderspitalgasse 15, A-1095 Wien, Austria
The objective of this longitudinal (3 year) study was to determine predictors of abstinence in 515 employees of a
steel plant (28% female, age 18–67 years) after participation in Allen Carr seminars (intensive group counselling in asingle session of 6 h). Answers given in computer aided phone interviews were analysed by stepwise and Coxregression. Of 510 responding persons 262 (51.4%) reported continuing abstinence. In a random sample of 61respondents cotinine concentration in urine was measured, showing high agreement with smoking history. Socialsupport increased abstinence, which was more persistent in males and office workers. Also in female participants thenon-smoking spouse was a significant predictor for abstinence while a higher body weight predicted relapse.
Addictive Behaviors xx (2006) xxx – xxx
Long term success of short smoking cessation seminars
Department of Preventive Medicine, Institute of Environmental Health, Medical University of Vienna,
Kinderspitalgasse 15, A-1095 Wien, Austria
The objective of this longitudinal (3 year) study was to determine predictors of abstinence in 515 employees of a
steel plant (28% female, age 18–67 years) after participation in Allen Carr seminars (intensive group counselling in asingle session of 6 h). Answers given in computer aided phone interviews were analysed by stepwise and Coxregression. Of 510 responding persons 262 (51.4%) reported continuing abstinence. In a random sample of 61respondents cotinine concentration in urine was measured, showing high agreement with smoking history. Socialsupport increased abstinence, which was more persistent in males and office workers. Also in female participants thenon-smoking spouse was a significant predictor for abstinence while a higher body weight predicted relapse.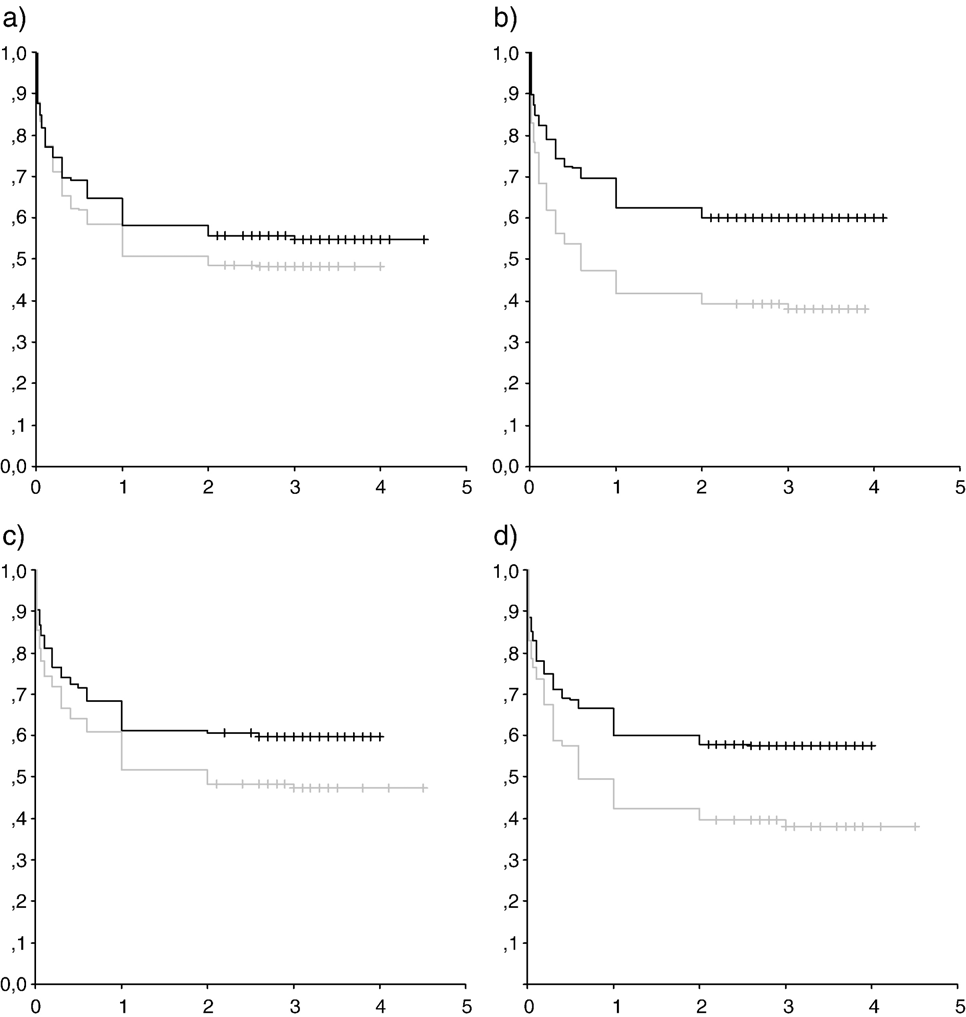 H. Moshammer, M. Neuberger / Addictive Behaviors xx (2006) xxx–xxx
Fig. 1. Kaplan–Meier plots of abstinence rate over 1500 days each: a) White collar workers (black) versus blue collar workers(grey); b) Non-smoking spouse / partner (black) versus smoking spouse / partner (grey); c) More than 6 participants at theseminars from the same work-place (black) versus 6 or less participants (grey); d) Poor health (3–5) before the seminar (black)versus good health (1 and 2, grey). Y-axis: percentage of non-smokers, X-axis: years.
H. Moshammer, M. Neuberger / Addictive Behaviors xx (2006) xxx–xxx
Fig. 1. Kaplan–Meier plots of abstinence rate over 1500 days each: a) White collar workers (black) versus blue collar workers(grey); b) Non-smoking spouse / partner (black) versus smoking spouse / partner (grey); c) More than 6 participants at theseminars from the same work-place (black) versus 6 or less participants (grey); d) Poor health (3–5) before the seminar (black)versus good health (1 and 2, grey). Y-axis: percentage of non-smokers, X-axis: years.