World J. Surg. 24, 1312–1318, 2000 DOI: 10.1007/s002680010217 Is the New Classification of Neuroendocrine Pancreatic Tumors of Clinical Help?
Martin Schindl, M.D.,1 Klaus Kaczirek, M.D.,1 Klaus Kaserer, M.D.,2 Bruno Niederle, M.D.1
1Department of Surgery, Division of General Surgery, Section of Endocrine Surgery, University of Vienna Medical School, Wa¨hringer Gu¨rtel
2Institute of Clinical Pathology, University of Vienna Medical School, Währinger Gu¨rtel 18-20, A 1090 Vienna, Austria
Abstract. A new concept of classifying neuroendocrine pancreatic tumors
atic tumors on the basis of clinicopathologic patterns was devel-
based on clinicopathologic patterns was summarized recently. To evaluate
oped by an experienced group of pathologists over the last decade
the clinical reliability and prognostic specificity of this classification system, 100 neuroendocrine pancreatic tumors were retrospectively cate-
[7–12]. Founded on their work, the objective of the current study
gorized as “benign,” “uncertain,” and “malignant” based on tumor risk
was to determine the clinical reliability and prognostic specificity
factors (size, local invasion and angioinvasion, cell atypia, metastases)
of this classification system by retrospectively analyzing the clini-
and were followed for disease recurrence and progression. Altogether, 71
cal course and survival with respect to “benign,” “malignant,” and
functioning tumors (insulinoma, gastrinoma, glucagonoma, enterochro-
“uncertain” tumors. Especially a therapeutic concept of tumors
maffin-like (ECL)oma, somatostatinoma) and 29 nonfunctioning neu- roendocrine pancreatic tumors (NETs) were studied. NETs had an in-
classified as “uncertain” and “malignant” should be developed. creased risk of malignancy (p < 0.05). Tumor size, gross invasion, and metastases correlated significantly with tumor behavior and allowed us to distinguish between “benign” and “malignant” tumors. About 89% of the Patients and Methods tumors < 20 mm were “benign,” whereas 71% > 20 mm were “malignant” (p < 0.05). In patients with “benign” and “uncertain” neuroendocrine pancreatic tumors, neither recurrence nor progression of disease was seen. About 41% of the patients with “malignant” tumors died of the
The medical documentation of 100 consecutive patients (47
disease. The 5-year estimated cumulative survival of those with “benign”
males, 53 females; mean age at operation 49.5 Ϯ 15.8 yeas, range
and “uncertain” tumors was 100% and 52 ؎ 10% for those with “malig- nant” tumors (p < 0.05). Histomorphologic details classifying the behav-
12–80 years) with a histologically verified neuroendocrine pancre-
ior of an “uncertain” tumor are known only after initial treatment and
atic tumor treated at the Department of Surgery, University of
definitive histopathologic investigation. Thus this information is of lim-
Vienna, Austria, were retrospectively reviewed. Information con-
ited clinical help for treatment strategies.
cerning preoperative history, disease-related symptoms, and lab-
oratory values was obtained from the patients’ reports. Special
emphasis was placed on disease-related symptoms, tumor size and
location in the pancreas, histopathology and evidence of regional
Since the first classification of gut neuroendocrine tumors by
or distant tumor spread, and type of operation.
William and Sandler in 1963, a variety of divergent nomenclature
systems to classify neuroendocrine histomorphology and predict
biologic behavior have been developed. The knowledge of cell
biology and tumorigenesis of the neuroendocrine cell system in-
creased over the last few decades, but classifications used so far
In each case diagnosis was made by clinical, biochemical, and
have not consider clinical, morphologic, and biologic features of
histopathologic analysis. Neoplasms were named functioning neu-
roendocrine tumors (FETs) according to their leading clinically
Pancreatic neuroendocrine tumors consist of tumor entities
and endocrine profiles. Those neoplasms lacking endocrine symp-
with clinical and pathologically distinct profiles. For these tumors,
toms were labeled nonfunctioning neuroendocrine tumors
it was shown that the presence of a specific endocrine hyperfunc-
tion syndrome, indicating a certain tumor entity, is at least of the
Tumor specimens were stained routinely with hematoxylin-
same importance for predicting biologic behavior as purely patho-
eosin. Neuroendocrine differentiation was identified by silver im-
pregnation techniques and immunstaining for neuroendocrine
The concept of classifying neuroendocrine gastroenteropancre-
markers, such as neuron-specific enolase (NSE), human islet cell
antibody (HISL-19), and chromogranin A, and for insulin, gastrin,
serotonin, pancreatic polypeptide (PP), and glucagon.
This International Association of Endocrine Surgeons (IAES) article
The FETs and NETs were classified in the same manner as
was presented at the 38th World Congress of Surgery International Sur-
gical Week (ISW99), Vienna, Austria, August 15–20, 1999.
“benign,” “uncertain,” and “malignant” based on known tumor-
Correspondence to: B. Niederle, M.D.
specific risk factors, such as tumor size, local invasion of surround-
Schindl et al.: Classification of Neuroendocrine Pancreatic Tumors Table 1. Tumor-specific risk factors: size, histomorphology, metastases.
advanced disease, additional examinations with chest roentgeno-
gram, abdominal CT, and somatostatin receptor scintigraphy were
For the definition of tumor-specific risk factors (size, local inva-
sion, gross invasion, angioinvasion, cell atypia, regional and dis-
tant metastasis), a statistical analysis using the Mann-Whitney
U-test and the linear-by-linear association test were performed
(p Ͻ 0.05). The outcome was determined by evidence of local
ing tissue, angioinvasion, histomorphologic differentiation (cell
tumor recurrence and progression of disease (distant tumor
and tissue atypia, mitotic activity), and evidence of regional and
spread, disease-related death). The cumulative 5- and 10-year
distant metastases as proposed recently (Table 1) [12].
survival rates were estimated by the Kaplan Meier method with
All pancreatic neuroendocrine tumors Յ 20 mm in largest
significance according to the log-rank test at a probability of p Ͻ
diameter without local invasion or angioinvasion and no evidence
of regional lymphatic or distant metastases were classified as
“benign.” Tumors confined to the pancreas and without metasta-
ses were said to be “uncertain” if the tumor size was Ͼ 20 mm or
local invasion had occurred (or both). Tumors with extended
invasion of peripancreatic tissue or regional or distant tumor
spread were classified as “malignant” (Table 1).
The 71 tumors were composed of endocrine cells of either ortho-
Preoperative Evaluation and Surgical Treatment
topic or ectopic origin, leading to an endocrine syndrome (FET):
52 insulinomas, 11 gastrinomas, 3 glucagonomas, 2 somatostati-
Tumor size, local extension, and distant spread were evaluated
nomas, 2 vasoactive intestinal peptide-secreting tumor (VIPoma),
preoperatively using computed tomography (CT) or magnetic
and 1 enterochromaffin-like (ECL)oma. In the following analysis
resonance tomography (MRT). Ultrasonography was performed
glucagonomas, somatostatinomas, VIPomas, and ECLoma were
intraoperatively to localize tumors not detected preoperatively, to
summarized as “other functioning neuroendocrine pancreatic tu-
exclude multiple endocrine tumors, and to determine the tumor’s
mors” (OFET) (n ϭ 8). A group of 29 neuroendocrine tumors,
although immunoreactive for various hormones, were lacking any
All patients underwent primary surgery with the intent to cure
(n ϭ 83) or to debulk the tumor in patients with preoperatively
verified liver metastases (n ϭ 17). The indications for surgery
were a well defined clinical syndrome (n ϭ 71) or symptoms of the
pancreatic tumor itself (n ϭ 29).
The distribution of tumor size was different among the tumor
Independent the tumor size, radical removal of the primary
entities: Gastrinomas, OFETs, and NETs were large, with mean
tumor by a local limited approach (enucleation) was performed if
diameters of 56.2 Ϯ 53.9 mm (range 10–200 mm), 91.4 Ϯ 39.3 mm
feasible. If enucleation was technically impossible (close to the
(range 40–150 mm), and 50.6 Ϯ 19.9 mm (range 21–100 mm),
pancreatic duct, gross tumor invasion), extended surgery (pancre-
respectively; whereas insulinomas were small, with a mean diam-
atic resection) was done. If diagnosed, regional lymph nodes
eter of 18.5 Ϯ 12.9 mm (range 3–80 mm). On histomorphologic
metastases were removed by systematic lymph node dissection.
examinations local invasion and angioinvasion were evident in
Systemic chemotherapy, biotherapy, and somatostatin analogs
20% (10/51) and 14% (7/51) of insulinomas, 82% (9/11) and 45%
were not used routinely. In case of liver metastasis at the time of
(5/11) of gastrinomas, 63% (5/8) and 38% (3/8) of OFETs, and
diagnosis or follow-up, hepatic arterial embolization was recom-
62% (18/29) and 52% (15/29) of NETs, respectively. Tumor spec-
mended. Adjuvant therapy was applied in these patients and in
imens were further examined for signs of cell and tissue atypia.
Mild to moderate cell and nucleus polymorphism, increased mi-
totic activity, and atypical tissue structures were evident in 12%
(6/51) of insulinomas, 55% (6/11) of gastrinomas, 38% (3/8) of
OFETs, and 62% (18/29) of NETs (Table 2).
Patients were followed over a mean postoperative period of
92.6 Ϯ 92.0 months (range 1–397 months). Complete follow-up
data were obtained for all 100 patients. Within the observation
Tumor Biology: Gross Local Invasion and Distant Tumor
period 40 patients (40%) died. The private physicians were asked
to report the clinical course of these patients, and the autopsy
protocols were studied retrospectively. Recent clinical data were
Gross local invasion into peripancreatic tissue, adrenal glands, or
collected from 56 living patients. Including a physical examina-
intestine at the time of operation was evident in 12% (6/51) of
tion, a medical questionnaire about disease-related symptoms and
insulinomas, 45% (5/11) of gastrinomas, 38% (3/8) of OFETs, and
an analysis of blood hormones in patients with an initial FET was
45% (13/29) of NETs. About 8% (4/51) of insulinomas also
performed. In cases of functional recurrence or in cases of initially
showed either lymphatic or distant tumor spread to other organs,
World J. Surg. Vol. 24, No. 11, November 2000 Table 2. Tumor pathology: size, local infiltration, histomorphologic differentiation, gross invasion, and distant tumor spread.
INS: insulinoma; GAS: gastrinoma; OFET: other functioning neuroendocrine pancreatic tumors; NET: nonfunctioning neuroendocrine pancreatic
aIn one patient with an insulinoma localized in the pancreatic head (10 mm) a nonfunctioning cystic neuroendocrine tumor of the pancreatic tail
was removed by tail resection during initial operation. Persistence of symptoms was due to failed removal of the functioning tumor in the pancreatic
head. This patient was excluded from further evaluations. Table 3. Clinicopathologic classification.
29/41 (71%) 27/41 (66%) 11/41 (27%) 17/41 (41%)
Table 4. Tumor risk factor analysis: tumor size, local tumor classification, and tumor spread.
*p Ͻ 0.05, Mann-Whitney U-test.
as did 64% (7/11) of gastrinomas, 50% (4/8) of OFETs and 45%
Tumor Size, Local Tumor Classification, Tumor Spread
In 44 patients the neuroendocrine pancreatic tumor was less than
20 mm. The tumor classification was benign in 39, uncertain in 4,
and malignant in 1 patient retrospectively. None of the 44 patients
showed lymph node or distant metastasis (Table 4).
Based on the recently defined clinicopathologic profile taking into
The other 56 tumors were larger than 20 mm, with 16 classified
as “uncertain” and 40 as “malignant” (Table 4). Altogether, 11 of
account the endocrine syndrome, size, histomorphology, and
the 40 malignant tumors had histologically verified lymph node
growth characteristics [12], 80 of 100 neuroendocrine pancreatic
metastases only, and 14 had lymph node and distant metastases
tumors were clearly assigned to either “benign” (n ϭ 39) or
“malignant” (n ϭ 41) tumor behavior. Benign behavior was as-
sumed in 39 well differentiated, small insulinomas without anysigns of advanced tumor growth at the time of operation, whereas
malignancy was obvious in 41 patients with either gross local
A total of 38 patients with “benign” classified pancreatic neuroen-
invasion to peripancreatic tissue (27/41, 66%) or local (11/41,
docrine tumors were treated by enucleation (n ϭ 30) or resection
27%) or distant (17/41, 41%) tumor spread (Table 3).
(n ϭ 8; seven tail resections, one hemipancreatectomy). In one
In 20 patients tumors were classified as having “uncertain”
patient a 10 mm insulinoma was missed in the pancreatic head. A
behavior. Although extensive tumor spread was not evident at the
20 mm “benign” cystic neuroendocrine tumor of the pancreatic
time of operation, tumors were thought at risk for malignant
tail was removed by tail resection (Table 5). Mean tumor size was
behavior because of a size larger than 20 mm (16/20, 80%), local
14.0 Ϯ 3.5 mm (range 8–20 mm) in the enucleation group and
pancreatic invasion (7/20, 35%) or angioinvasion (5/20, 25%), or
14.5 Ϯ 6.5 mm (range 3–20 mm) in the resection group.
atypical histomorphology (3/20, 15%) (Table 3).
Tumor enucleations were performed in 10 of 20 patients with
Altogether, 17 of 71 functioning tumors (24%) and 24 of 29
“uncertain” neoplasms. Mean tumor size was 23.4 Ϯ 11.1 mm
nonfunctioning tumors (83%) were classified as “malignant”
(range 10–45 mm). Local pancreatic invasion was shown in 30%
(Mann-Whitney U-test, p Ͻ 0.05).
(3/10) of the tumor specimens. In 30% (3/10) invasion of small
Schindl et al.: Classification of Neuroendocrine Pancreatic Tumors Table 5. Surgical treatment of benign, uncertain, and malignant classified pancreatic neuroendocrine tumors and follow-up results.
Numbers in parentheses are palliative surgical procedures (n ϭ 19) done because of extended gross invasion (n ϭ 2) or bilateral liver metastases
LR: local recurrence of disease; DR: distant recurrence of disease; DD: died of disease. aFive patients with biliodigestive and/or gastroenteric anastomoses.
vascular structures was evident. In 10 patients tumors were re-
progressive disease. Four patients (10%) died of unrelated disease
moved completely by resection (nine tail resections, one Whipple
free of tumor 48.6 Ϯ 88.5 months after surgery, and six patients
resection) (Table 5). Mean tumor size was 60.6 Ϯ 43.8 mm (range
(15%) are alive less than 3 months after surgery.
15–150 mm). At pathologic examination, 40% (4/10) showed local
Recurrence of disease was seen in 4 of 19 patients (18%) with
invasion of the pancreatic tissue, and 30% (3/10) had angioinva-
radically treated “malignant” pancreatic neuroendocrine tumors.
In one patient a NET recurred locally 5 months after the Whipple
In 2 of 41 patients the “malignant” pancreatic neuroendocrine
procedure, and distant recurrence in the liver was seen in three
tumor was enucleated. The tumor sizes were 11 and 30 mm,
patients (one gastrinoma 19 months after enucleation, and one
respectively. Gross local invasion of surrounding tissue was evi-
glucagonoma and one NET 8 and 34 months after pancreatic tail
dent in both patients, and there was evidence of angioinvasion and
resections, respectively). Three of these four patients died 66.3 Ϯ
regional tumor spread to lymph nodes in one of the two patients.
50.8 months (range 13–115 months) after the initial operation,
Various pancreatic left resections were performed in 17 patients
and one patient with liver metastases is still alive 107 months after
(14 tail resections, 3 hemipancreatectomies). Mean tumor size
enucleation of a pancreatic gastrinoma.
was 55.6 Ϯ 24.9 mm (range 21–110 mm). Of these tumors, 59%
Analysis of cumulative survival (Kaplan-Meier) showed differ-
(10/17) showed gross local invasion, 71% (12/17) angioinvasion,
ent survival rates depending on the tumor entity, tumor size, gross
and 35% (6/17) regional and 41% (7/17) distant tumor spread.
invasion, and regional or distant metastases. Patients with insuli-
The 12 neuroendocrine pancreatic tumors localized in the pan-
noma (INS) had an estimated 5-year survival of 97 Ϯ 3%, whereas
creatic head were resected by a Whipple procedure. Mean tumor
5-year survival estimation for patients with gastrinoma was 50 Ϯ
size was 47.3 Ϯ 13.9 mm (range 21–80 mm). Of these tumors,
18%, for those with OFET 83 Ϯ 15%, and for those with NET
67% (8/12) showed gross local invasion, 58% (7/12) angioinvasion,
63 Ϯ 11% (Fig. 1A). This difference was statistically significant
and 25% (3/12) regional and 17% (2/12) distant tumor spread.
(INS vs. OFET p Ͻ 0.05; INS vs. GAS and NET p Ͻ 0.001).
Ten malignant tumors (10/41; 24%) were not removed because of
Estimated survival in patients with tumors smaller 20 mm was
extended invasion into adjacent organs (n ϭ 1), extended gross
100%; it decreased among those with larger tumors to 68 Ϯ 8% at
local invasion in combination with extended lymph node involve-
5 years (p Ͻ 0.001) (Fig. 1B). The evidence of peripancreatic gross
ment (n ϭ 1), or extended bilateral liver metastases (n ϭ 8). In 5
invasion, lymph nodes, and distant metastasis decreased the
of these 10 patients palliative biliodigestive, gastro-enteric anas-
5-year survival to 44 Ϯ 11%, 78 Ϯ 14%, and 20 Ϯ 12% respec-
tomoses, or both were performed at the initial exploration (Table
tively (p Ͻ 0.001) (figures not shown). “Benign” and “uncertain”
5). Mean tumor diameter was 61.4 Ϯ 38.8 mm (range 25–80 mm).
pancreatic neuroendocrine tumors had 5- and 10-year survival
rates of 100%, whereas the estimated survivals for those with
“malignant” tumors decreased to 52 Ϯ 10% and 27 Ϯ 13%
respectively (p Ͻ 0.001) (Fig. 1C).
All patients were followed over time for tumor recurrence or
progression. The mean Ϯ SD follow-up was 92.6 Ϯ 92.0 months
Discussion
Among the patients with “benign” (follow-up 111.4 Ϯ 102.2
After the first description of neuroendocrine cells in pancreatic
months) and “uncertain” (follow-up 134.7 Ϯ 98.0 months) pan-
islets by Paul Langerhans in 1869 and introduction of the term
creatic neuroendocrine tumors, neither recurrence nor progres-
“carcinoid” by Oberndorfer in 1907, it took a long time for today’s
sion of disease was seen at any time during follow-up. Two
concept of neuroendocrine gastroenteropancreatic tumors to be-
patients with benign insulinomas had persistent endocrine symp-
come established. In 1980 the World Health Organization
toms after incomplete or failed tumor removal at the initial
(WHO) classification of endocrine tumors applied the term “car-
cinoid” to all tumors of the diffuse neuroendocrine system but
Of 41 patients (41%) with “malignant” tumors, 17 died of
excluded pancreatic endocrine tumors, which were separately cat-
disease 43.0 Ϯ 42.2 months (range 1–159 months) after surgery;
egorized as “islet cell tumors.” During the last 10 years, with
14 patients (34%) are still alive, 8 without (follow-up 42.1 Ϯ 29.7
advancing knowledge of neuroendocrine histogenesis and neo-
months) and 6 with (follow-up 56.6 Ϯ 37.3 months) recurrent or
plastic proliferation, pancreatic endocrine tumors were included
World J. Surg. Vol. 24, No. 11, November 2000
in the group of “neuroendocrine tumors” and were distinguished
according to clinical and histomorphologic tumor patterns. A new
classification system was first published in 1994 as the “revised
classification system of neuroendocrine tumors,” following the
need to encompass the entire spectrum of behavior-predicting
morphologic and clinical parameters [11]. Its main focus was on
constituting a comparable classification and estimating neoplastic
behavior by combining clinicopathologic tumor profiles, including
endocrine hyperfunction-related symptoms, tumor size, growth
characteristics, histomorphologic differentiation, and evidence of
distant tumor growth. To our knowledge there is no experience
with the clinical reliability of this new, recently established classi-
fication of neuroendocrine pancreatic tumors.
In our series, 71 of 100 neuroendocrine pancreatic tumors were
diagnosed because of a biochemically defined clinical syndrome.
Of the functioning neoplasms, 17 (24%) were classified “malig-
nant” because they showed gross peripancreatic and angioinva-
sion, cell atypia, or metastases to regional lymph nodes, liver, or
other distant sites. There was a statistically significant difference
from nonfunctioning tumors, with 24 of 29 (83%) (p Ͻ 0.05)
showing malignant behavior. Independent of the surgical proce-
dure, there was a significant difference in 5- and 10-year estimated
cumulative survival rates of functioning (88 Ϯ 5%, 84 Ϯ 6%) and
nonfunctioning (63 Ϯ 11%, 49 Ϯ 12%) neuroendocrine pancre-
Nonfunctional pancreatic tumors comprise a higher risk of
malignancy compared to tumors producing a hyperfunctional syn-
drome [13]. La Rosa et al. found eight morphologic variables in
nonfunctioning neuroendocrine pancreatic tumors that were sig-
nificantly related to malignancy: tumor size, local pancreatic in-
vasion, vascular microinvasion, perineural microinvasion, mitosis,
nuclear atypia, Ki67 proliferation index, and progesterone recep-
tor expression. Among these variables vascular/perineural micro-
invasion and the Ki67 proliferative index were the most sensitive
and specific and were used by the authors to further distinguish
neoplasms with and without increased risk of malignancy [14].
Ectopic cell type tumors (e.g., gastrinoma, vipoma) contain an
additional risk of malignancy [3, 7, 8]. In our series only 5 of 52
insulinomas (10%) compared to 7 of 11 gastrinomas (64%) (p Ͻ
0.05) were classified “malignant.” Although evidence exists that
the type of endocrine hyperfunction syndrome influences tumor
behavior, its relation to morphologic factors remains to be deter-
mined [1, 6, 15]. An explanation for the better clinical outcome of
functioning tumors in our series could be the large number of
small (Ͻ 20 mm) insulinomas. Usually, insulinomas with their
typical clinical symptoms are diagnosed earlier than other func-
tioning or nonfunctioning tumors, which are recognized late in
their clinical course, sometimes in a large and metastatic state
Among various factors contributing to the development of dis-
tant metastases, one of the criteria for determining malignancy
Š Fig. 1. Kaplan-Meier cumulative survival of patients with neuroendo-
crine pancreatic tumors. Number of patients at risk is indicated on top of
the curves. A. Survival of various tumor entities (*p Ͻ 0.001, §p ϭ 0.03). B.
Tumor size Յ 20 mm versus Ͼ 20 mm (p Ͻ 0.001). C. Classification
“benign” versus “uncertain” versus “malignant” (p Ͻ 0.001). INS: insuli-
noma; OFET: other functioning neuroendocrine pancreatic tumors; GAS:
Schindl et al.: Classification of Neuroendocrine Pancreatic Tumors
was found by Weber and coworkers [16] in patients with gastri-
was performed in two patients: One patient died 10 months
nomas, indicating a significant correlation between primary tumor
postoperatively of progressive disease, and one is still alive at 96
size and the occurrence of distant metastases. In contrast, no
months. After several liver embolizations the patient is on inter-
correlation was found between tumor size and regional lymph
node metastases. Size is an important but not independent prog-
Because of extended gross invasive growth, multiple distant
nostic factor [14]. In our series tumors less than 20 mm had a
metastases, or both, 10 tumors were left in situ. Bypass procedures
better estimated cumulative survival than tumors with a diameter
were useful for five neuroendocrine pancreatic tumors localized in
larger than 20 mm. The probability of malignant behavior, indi-
the pancreatic head. The cumulative survival rate of these patients
cated by gross invasion and distant metastases, significantly in-
was 56 Ϯ 17% after 1 year. The maximal life expectancy was 4
creases in tumors larger than 20 mm, in the same way as the
years. In contrast, in patients with surgical tumor debulking the
incidence of extended angioinvasion and histomorphologic atypia
1-year cumulative survival was 88 Ϯ 20%, and one patient is still
intensifies. Of 44 tumors less than 20 mm, 39 were classified
“benign,” 4 as “uncertain,” and one as “malignant.” In contrast,
A total of 39 insulin-producing tumors assessed “benign” intra-
for 16 of 56 tumors larger than 20 mm the clinical behavior was
operatively were removed by tumor enucleations or limited pan-
predicted as “uncertain” and in 40 “malignant.” At the time of
creatic tail resections. The clinico-pathologic classification con-
initial surgery 25 of the 40 “malignant” tumors had histologically
firmed the “benign” behavior. In 20 patients an “uncertain”
verified lymph node and distant metastases.
outcome was predicted retrospectively; 10 of these 20 tumors,
According to studies of Heitz et al., Creutzfeld, Solcia et al., and
mainly localized in the pancreatic head with a tumor diameter
Klo¨ppel and Heitz, the functional status of tumor cells, size, and
between 10 and 45 mm were removed by enucleation. Nine tu-
differentiation must be assessed for an appropriate prognostic
mors localized in the pancreatic body or tail with a diameter of 22
evaluation of neuroendocrine pancreatic tumors [3, 7, 9, 17].
to 150 mm were removed by pancreatic body or tail resection, and
Intraoperatively, the size of the tumor, gross invasion of adjacent
one 50 mm pancreatic head tumor was removed by a Whipple
tissue, and distant metastases can be recognized macroscopically.
procedure. At least half of these tumors classified as “uncertain”
Lymph node metastases can be diagnosed with the help of frozen
were successfully removed by a local limited surgical approach.
sections. Other histomorphologic characteristics of an “uncertain”
Within the follow-up period none of these patients developed
or “malignant” behavior, such as local infiltration, extended an-
local or distant recurrences. Theoretically, these 10 patients (6
gioinvasion, or cell atypia, are verified only after detailed micro-
insulinoma, 3 gastrinoma, 1 NET) are at risk of disease progres-
scopically investigations [13, 14, 18].
sion. Nevertheless, we would not advise reoperation or adjuvant
All but one “malignant” tumor could be easily distinguished
from “benign” neoplasms. This 11 mm insulinoma, which macro-
scopically was classified as “benign” and which was easily enucle-
Conclusions
ated from the pancreatic head, was classified as a tumor with
predicted “malignant” behavior by its definitive histology because
Knowledge of endocrine function, tumor size, gross invasion, and
of local pancreatic invasion and cell atypia. Six months later the
metastases allows us to distinguish between neuroendocrine pan-
patient is biochemically and clinically free of disease without
creatic tumors with “benign” or “malignant” behavior in most
patients. Depending on the size and localization in the pancreas,
Except one patient with a 30 mm gastrinoma enucleated from
enucleation or resection (with lymph node dissection for diagnos-
the pancreatic head and with a “picking” of two, retrospectively
tic and therapeutic purposes) should be performed. In selected
positive lymph nodes, malignancy was recognized during the ini-
cases with liver metastases even palliative enucleation or resection
tial operation in all other patients. Twenty tumors were removed
by radical pancreatic resection with systematic lymph node dis-
Histomorphologic details (local invasion, angioinvasion, cell
section. Palliative pancreatic resections were performed in nine
atypia) classifying an “uncertain” tumor behavior are known after
patients with bilateral liver metastases. The estimated cumulative
the initial treatment and definitive histopathologic investigations.
5- and 10-year survival rates were, respectively, 98.2 Ϯ 2% and
Thus this (retrospective) information is of limited help for treat-
92 Ϯ 5% for radically removed tumors and 53 Ϯ 18% and 35 Ϯ
ment strategies. Tumors with the clinicopathologic profile of an
18% for palliatively removed tumors (p Ͻ 0.001).
“uncertain” lesion are “at risk” of developing a malignant course
Distant metastases were associated with an impaired prognosis
and must therefore be followed carefully. Nevertheless, in none of
[19], whereas gross invasion or local lymph node metastases alone
our patients was reoperation necessary.
were not [5]. According to Thompson and Eckhauser [5] and
Grant [13], an aggressive surgical resection is warranted for tu-
Re´sume´
mors without distant metastases. Some of these tumors may be
cured by an appropriate pancreatic resection and systematic
Re´cemment, on a e´labore´ une nouvelle classification des tumeurs
lymph node dissection even when peripancreatic lymph nodes are
neuroendocrines du pancre´as, base´e sur le tableau clinico-
already involved. Grant reported a 5-year survival of 35% [13].
pathologique. Afin d’e´valuer la fiabilite´ clinique et la spe´cificite´
In some patients with functioning tumors, Surgical debulking of
pronostique de cette classification, on a cate´gorise´, re´tro-
the primary tumor is indicated even when a curative resection
spectivement, 100 tumeurs neuroendocrines du pancre´as en
cannot be accomplished. In these patients liver embolization can
«be´nigne», «incertaine» et «maligne», en se basant sur les facteurs
improve the quality of life and, in some respect, life expectancy
de risque tumoraux (taille, invasion locale et vasculaire, atypie
[20]. Although a Whipple procedure is not indicated when ex-
cellulaire, me´tastases) et sur le suivi (re´cidive et e´volution). On a
tended bilateral hepatic metastases are present [5], this procedure
e´tudie´ 71 tumeurs endocrines fonctionnelles (TEF): insulinome,
World J. Surg. Vol. 24, No. 11, November 2000
gastrinome, glucagonome, ECLome, somatostatinome, et 29
proporciona escasa ayuda en la planificacio´n de la estrategia
tumeurs endocrine non fonctionnelles (TEN). Le risque de
malignite´ e´tait plus e´leve´ en cas de TEN (p Ͻ 0.05). La taille
tumorale, l’invasion macroscopique et les me´tastases corre´laient
de fac¸on significative avec l’e´volution tumorale et a permis de
References
distinguer les tumeurs «be´nignes» et «malignes». Ainsi, 89% des
tumeurs de diame`tre Յ 20mm e´taient be´nignes, alors que 71%
1. Larsson, L.I.: Endocrine pancreatic tumors. Hum. Pathol. 9:401, 1978
2. Modlin, I.M.: Endocrine tumors of the pancreas. Surg. Gynecol.
des tumeurs de diame`tre Ͼ 20mm e´taient malignes (p Ͻ 0.05).
Chez le patient ayant une tumeur classe´e «be´nigne» ou
3. Heitz, P.U., Kasper, M., Polak, J.M., Klo¨ppel, G.: Pancreatic endo-
«incertaine», on n’a jamais observe´ ni re´cidive ni progression
crine tumors. Hum. Pathol. 13:263, 1982
tumorale. Parmi les patients ayant une tumeur maligne, 41% sont
4. Mukai, K., Grotting, J.C., Greider, M.H., Rosai, J.: Retrospective
de´ce´de´s de leur maladie. La survie cumulative estime´e a` 5 ans des
study of 77 pancreatic endocrine tumors using the immunoperoxidase
method. Am. J. Surg. Pathol. 6:387, 1982
tumeurs «be´nignes» et «incertaines», d’une part, et des tumeurs
5. Thompson, N.W., Eckhauser, F.E.: Malignant islet-cell tumors of the
«malignes», d’autre part, a e´te´, respectivement, de 100% et de
pancreas. World J. Surg. 8:940, 1984
52 Ϯ 10% (p Ͻ 0.05). Les caracte´ristiques histomorphologiques
6. Broughan, T.A., Leslie, J.D., Soto, J.M., Hermann, R.E.: Pancreatic
pour classer les tumeurs «incertaines» ne sont connus en fait
islet cell tumors. Surgery 99:671, 1986
7. Klo¨ppel, G., Heitz, P.U.: Pancreatic endocrine tumors. Pathol. Res.
qu’apre`s traitement initial et examen histopathologique de´finitif.
Ainsi cette information est de peu de secours clinique pour le
8. Solcia, E., Sessa, F., Rindi, G., Villani, L., Riva, C., Buffa, R., Capella,
C.: Classification and histogenesis of gastroenteropancreatic endo-
crine tumours. Eur. J. Clin. Invest. 20(Suppl. 1):S72, 1990
9. Solcia, E., Sessa, F., Rindi, G., Bonato, M., Capella, C.: Pancreatic
endocrine tumors: general concepts; nonfunctioning tumors and tu-
mors with uncommon function. In Endocrine Pathology of the Gut
Recientemente y apoya´ndose en el patro´n anatomoclı´nico se ha
and Pancreas, Dayal, Y., editor, Boca Raton, CRC Press, 1991, p. 105
descrito una nueva clasificacio´n de los tumores neuroendocrinos
10. Klo¨ppel, G., Heitz, P.U.: Classification of normal and neoplastic
del pa´ncreas. Para evaluar la realidad clı´nica y el valor prono´stico
neuroendocrine cells. Ann. N.Y. Acad. Sci. 733:19, 1994
11. Capella, C., Heitz, P.U., Ho¨fler, H., Solcia, E., Klo¨ppel, G.: Revised
de esta clasificacio´n se efectu´a un estudio retrospectivo de 100
classification of neuroendocrine tumors of the lung, pancreas and gut.
tumores neuroendocrinos de pa´ncreas. Basados en los factores
tumorales de riesgo (taman˜o, localizacio´n, invasio´n vascular,
12. Rindi, G., Capella, C., Solcia, E.: Cell biology, clinicopathological
atipia celular y meta´stasis), ası´como en la recidiva y progresio´n de
profile, and classification of gastro-enteropancreatic endocrine tu-
la enfermedad, se dividieron dichos tumores en 3 categorı´as:
13. Grant, C.S.: Surgical management of malignant islet cell tumors.
benignos, de prono´stico incierto y malignos. Se estudiaron 71
14. La Rosa, S., Sessa, F., Capella, C., Riva, C., Leone, B.E., Klersy, C.,
glucagonomas, eclomas y somatostatinomas, y 29 tumores no
Rindi, G., Solcia, E.: Prognostic criteria in nonfunctioning pancreatic
funcionantes (NET). Los NET tienen un mayor riesgo de
endocrine tumours. Virchows Arch. 429:323, 1996
15. Stefanini, P., Carboni, M., Patrassi, N., Basoli, A.: Beta-islet cell
malignizacio´n (p Ͻ 0.05). El taman˜o tumoral, la invasio´n
tumors of the pancreas: results of a study on 1,067 cases. Surgery
macrosco´pica y las meta´stasis se correlacionan exactamente con la
conducta tumoral, por lo que pueden diferenciarse perfectamente
16. Weber, H.C., Venzon, D.J., Lin, J.T., Fishbein, V.A., Orbuch, M.,
los tumores malignos de los benignos. El 89% de los tumores Յ 20
Strader, D.B., Gibril, F., Metz, D.C., Fraker, D.L., Norton, J.A.,
mm fueron benignos, mientras que el 71% Ͼ 20 mm fueron
Jensen, R.T.: Determinants of metastatic rate and survival in patients
with Zollinger-Ellison syndrome: a prospective long-term study. Gas-
malignos (p Ͻ 0.05). En ninguno de los pacientes con neoplasias
benignas o de prono´stico incierto se observaron recidivas o
17. Creutzfeldt, W.: Endocrine tumors of the pancreas. In The Diabetic
progresio´n de la enfermedad. Sin embargo, el 41% de los
Pancreas, Volk, B.W., Arquilla, E.R., editors, New York, Plenum,
pacientes con neoplasias malignas fallecieron a causa de su
18. Cubilla, A.L., Hajdu, S.I.: Islet cell carcinoma of the pancreas. Arch.
enfermedad. La supervivencia acumulativa a los 5 an˜os fue del
100% para los tumores benignos y de prono´stico incierto,
19. Johanson, V., Tisell, L.E., Olbe, L., Wa¨ngberg, B., Nilsson, O., Ahl-
mientras que para los malignos, oscilo´ alrededor del 52 Ϯ 10%
man, H.: Comparison of survival between malignant neuroendocrine
(p Ͻ 0.05). La clasificacio´n morfolo´gica de los tumores de
tumours of midgut and pancreatic origin. Br. J. Cancer 80:1259, 1999
prono´stico incierto se establece definitivamente tras el
20. Winkelbauer, F.W., Nierderle, B., Graf, O., Prokesch, R., Thurnher,
S., Wildling, R., Lammer, J.: Malignant insulinoma: permanent he-
tratamiento quiru´rgico inicial, puesto que exige una minuciosa
patic artery embolization of liver metastases—preliminary results.
investigacio´n histopatolo´gica. Por tanto, esta informacio´n
Cardiovasc. Intervent. Radiol. 18:353, 1995
This chapter is not intended to be a ªGuide for Authorsº such as those thatyou can find in any journal. Our main advice is: do not write the paperfirst in your own language and then translate it into English; instead, do itin English directly. When you have a subject that you want to report, first of all you needto look up references. You can refer to the Index Medicus (http://www.ncbi.nlm.nih.
 World J. Surg. 24, 1312–1318, 2000
World J. Surg. 24, 1312–1318, 2000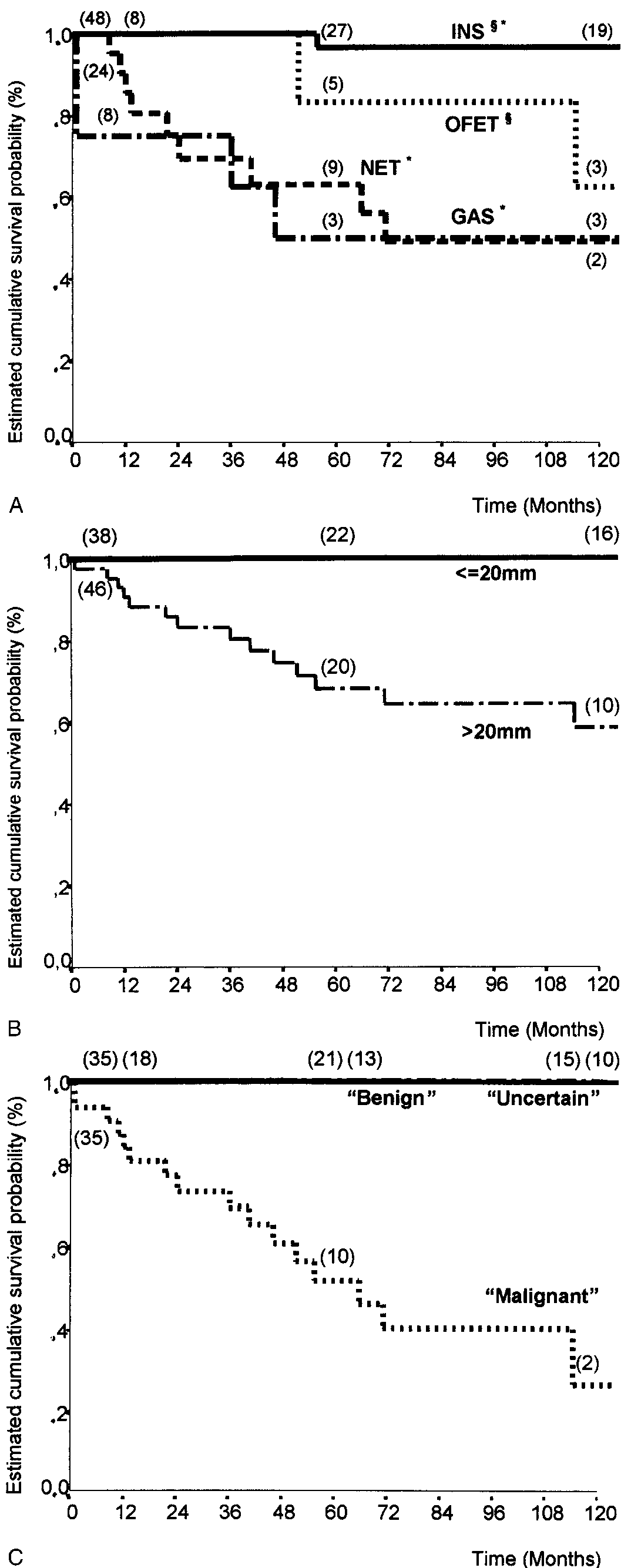 World J. Surg. Vol. 24, No. 11, November 2000
World J. Surg. Vol. 24, No. 11, November 2000