SECTION NINE DAHL-CHASE DIAGNOSTIC SERVICES NON-GYN CYTOLOGY Requisition Instructions for Non-Gyn Cytology Requisitions….………………………………….2 Requisitions
Cytology and Surgical Pathology (physician offices)………………………………………….3
Surgical, Bone Marrow, Flow Cytometry, Non-gyn Cytology (hospitals)……………………4
Specimen Collection Quick Reference Table……………….…….………………………………5-6 Fine Needle Aspirations General Information………………….……………………………………7 A Physicians Guide to Fine Needle Aspiration Biopsy…………….………………….…….8-18 Detailed Collection and Submission Requirements Bladder Wash………………………………………………………………………………….19 Body Fluids…………………………………………………………………………………….19
Pleural, Pericardial, Abdominal, Synovial
Bronchoscopy Specimens…………………………………………………………….…….20
Bronchial Brush Bronchial Wash Bronchial Trap Brocho Alveolar Lavage Wang from Bronchoscopy Specimens for Special Stains…………………………………………………….……20
GMS Pneumocystis GMS Fungus AFB for mycobacteria Iron Stain for hemosiderin-laden macrophages Fat Stain for lipid laden macrophages
CSF and Vitreous Fluid…………….……………………………………………………….21 Gastrointestinal Tract Brushing……………………………………………………….……21 Nipple Discharge……………………….…………………………………………………….21 Sputum……………….………………………………………………………….………………22 Tzanck Prep for Herpes………………………………………………………………………22 Urine……………………………………………………………………………………….…….22 Guidelines for Shipping………………………………………………………………………….….23 Guidelines for Preservation……………………………………………………………….……….23 Anal Screening Protocol (Anal Pap and Anal HPV)…………………………………………….24 Unacceptable Specimens, Turn Around Time, Hours of Operation…………………….25 SECTION NINE DAHL-CHASE DIAGNOSTIC SERVICES NON-GYN CYTOLOGY CLIENT NON-GYN CYTOLOGY REQUISITION FORM INSTRUCTIONS Purpose:
To aid the clients in the completion of the non-gyn cytology requisition form. Procedure:
1. There are 2 available requisitions for non-gyn cytology specimens. Samples of these two
requisitions follow this procedure. Which requisitions you use will depend on the types of specimens you send from your facility:
a. All offices that send pap testing should use the "Cytology, Surgical, and Molecular
b. The "Surgical, Bone Marrow, Flow Cytometry, Non-Gyn Cytology Requisition" should be
used by all hospitals or offices that perform a variety of these procedures.
2. Enter the patient's last name, first name and middle initial (see note below if attaching
3. Fill out the removable label(s) at the top of the requisition with the patient's full name, 2nd
identifier (date of birth or MR#), and specimen source.
4. Enter the patient's date of birth. 5. Enter the gender of the patient as Male or Female. 6. Enter the patient's telephone number (if available). 7. Enter the patient's social security number. 8. Enter the medical record number if the specimen is coming from a hospital or office requiring a
9. Enter the street address and the city, State and zip code. 10. Enter the requesting physician's FULL name. 11. Enter the hospital / clinic / or physician's office name. 12. Enter the collection date and time. 13. Enter the name of the person completing this requisition. This will help if we need to call to verify
14. Enter the insurance numbers (include the policy number and group number) and the address of
the insurance. Please keep in mind that many insurance companies have multiple addresses so in order for us to bill the insurance, we will need the address. A photocopy of the insurance card is preferred.
15. Enter any additional physician's FULL name that would like a copy of the report. 16. If correlation with a previous or concurrent biopsy is requested please check the box to the right
and provide the previous accession number if available.
17. Enter the Clinical Information section and fill in the remaining areas based on the type of
• Minimum requirement for labeling of specimens and slides is the patient's FULL name, 2nd
identifier (DOB or MR#), and source of specimen. The exact spelling of the patient's name should agree with the requisition. Any discrepancies will need to be resolved before we will process the specimen.
• Please note that if your office would like to send a demographic sheet along with the
requisition, the following needs to be filled in on the requisition: The patient's full name, the date of birth, the physician's full name and location, and the collection date and time. The rest of the demographic information, we will take from the demographic sheet.
SECTION NINE DAHL-CHASE DIAGNOSTIC SERVICES NON-GYN CYTOLOGY COLLECTION TECHNIQUES FOR NON-GYNECOLOGIC CYTOLOGY
Specimens for Cytology may be held at room temperature, however, if there will be a delay of more than 24 hours before transport, then the specimen must be refrigerated. The Cytology fixative is CytoRich Red Solution. This is an alcohol-based fixative. Do not put Cytology specimens in formalin.
All specimens must be labeled with a minimum of the patient's full name, second identifier (DOB or MR#) and the source of the specimen. Slides are to be labeled on the frosted end in #2 pencil with the full patient name, second identifier (DOB or MR#), and source. Do not send unlabeled slides in a labeled container. Keep in mind that the source on the requisition and the source on the specimen must agree. Please send completed Non Gyn Cytology Request Form with the specimen. All supplies may be ordered through Dahl-Chase Diagnostic Services Purchasing (941-8202 or 1-800-464-2332) SPECIMEN COLLECTION TECHNIQUE Body Fluids
Agitate container and pour 60mls of fluid into pre-filled
CytoRich Red container. If less than 50mls of fluid is available,
make 50:50 mix of specimen to CytoRich Red.
If additional fluid remains, pour 60mls into a sterile container
with a tight lid and send unfixed (refrigerated).
If additional fluid remains, send up to two more pre-filled
Label all containers with the patient's FULL name, 2nd
identifier (DOB or MR#), and source of specimen
Any remaining fluid should be kept refrigerated at the hospital
Bronchoscopy:
Put specimen into CytoRich Red Solution.
Label all containers with the patient's FULL name, 2nd
identifier (DOB or MR#), and source of specimen
Direct smears may be made for the WANG and fixed with
Specimens for Fat (Lipid) stain are to be FRESH. Do not put
Brushings:
Label slides with full patient name (pencil), second identifier
Prepare slides at time of collection by rolling brush across
glass slide, then fixing immediately with spray fixative or 95%
Vigorously swirl the brush for 15 seconds in CytoRich Red
Label container with patient's FULL name, 2nd identifier (DOB
Send at least 1ml CSF or vitreous fluid fresh refrigerated to
Cerebrospinal Fluid Vitreous Fluid
Label all containers with the patient's FULL name, 2nd
identifier (DOB or MR#), and source of specimen
Fine Needle Aspirations
Label slide with the patient's FULL name, 2nd identifier (DOB
Prepare direct smears and fix immediately with spray fixative
or place in 95% ethanol filled plastic container.
Rinse the needle in CytoRich Red solution container that is
also labeled with the patient's full name, second identifier (DOB or MR #) and source.
For detailed instructions, refer to the Physicians Guide to
Nipple Discharge
Label slide with the patient's FULL name, 2nd identifier (DOB
Express secretion on slide, fix immediately with cytology spray
Sputum for Cytology
Collect first morning specimens 3 days in a row for best results Patient may expectorate directly into CytoRich Red solution or
a fresh specimen may be collected in a sterile container and CytoRich Red may be added after receipt.
Label container with patient's FULL name, 2nd identifier (DOB
Tzanck Prep
Label slide with the patient's FULL name, 2nd identifier (DOB
Scrape base of vesicle with scalpel blade and smear onto
slide, spray fix immediately or fix with 95% ethanol.
Put 50/50 mix of urine into CytoRich Red Solution (not a first
Fix in CytoRich Red within 6 hours of collection if kept
Label container with the full patient name, second identifier
(DOB or MR#), and source of specimen (voided, catheterized, or bladder wash)
SECTION NINE DAHL-CHASE DIAGNOSTIC SERVICES NON-GYN CYTOLOGY FINE NEEDLE ASPIRATION BIOPSY GENERAL INFORMATION Fine Needle Aspiration Biopsy Fine needle aspiration (FNA) biopsy of superficial palpable lesions Principle:
Fine needle aspiration biopsy is a minimally invasive, cost effective procedure that procures cellular material for diagnosis using suction or non-suction techniques with a fine needle, usually23 gauge and above. Possible superficial palpable sites include breast, thyroid, parotid, and neck among others.
The accuracy of FNAB depends upon the site and type of lesion sampled, the operator's experience, the quality of specimen preparation, and the pathologist's diagnostic skills.
Refer to the physician guide on pages 9.9-9.19 for detailed instructions. Deep organ fine needle aspiration Principle:
Cytologic studies are performed on deep organ FNA (lung, kidney, pancreas, liver, adrenal gland, or abdominal mass) by FNA to detect neoplasia or exclude malignancy or infection. Collection and Submission: 1. These aspirations require visualization usually from CAT scan, but may also be done by
Fluoroscopy and Sonography. The radiologist or pulmonologist obtains them.
2. Material collected in the syringe is expelled onto a glass slide in a single drop and
smeared with another slide. The slides are immediately fixed with 95% ethanol or cytology spray fixative. The needle may then be rinsed in Cytorich Red solution. 3. A Rotex needle may also be used to sample the lesion. The Rotex needle should be
quickly wiped onto a slide after the specimen is collected. The slide should be fixed immediately. 4. Two slides may be made if there is enough material. 5. If a quantity of fluid is obtained at aspiration then it may also be submitted to the lab for
further processing by adding it to Cytorich Red solution.
6. The slides and/or Cytorich Red solution are labeled with the patient's full name, second
identifier (DOB or MR#), and source, and are sent to Dahl-Chase Diagnostic Services accompanied by a completed Non-Gyn Cytology Request Form.
7. Immediate adequacy assessment of the specimen by a cytotechnologist or pathologist is
available when prescheduled by calling Dahl-Chase Diagnostic Services at 973-7610. If the lesion is suspected to be a lymphoma, then specimen should be put into Flow Cytometry RPMI media (orange topped tube) and submitted to Flow Cytometry.
8. If the lesion is suspected to be inflammatory, then an additional needle pass should be
taken and all material can be expressed into sterile container and submitted to microbiology.
SECTION NINE DAHL-CHASE DIAGNOSTIC SERVICES NON-GYN CYTOLOGY FINE NEEDLE ASPIRATION PHYSICIAN GUIDE GENERAL STATEMENT……………………………………………………………….9 PRE-PROCEDURE CONSIDERATIONS………………………………………………9 Work PATIENT PREPARATION AND CONSENT………………………………………….10-11 ANESTHESIA…………………………………………………………………………….11 PROCEDURE…………………………………………………………………………….11 Materials
SPECIAL CONSIDERATIONS………………………………………………………….15 Lymph
PATIENT INSTRUCTIONS………………………………………………………………17-18 SPECIMEN SUBMISSIONS…………………………………………………………….18 RESULTS………………………………………………………………………………….18 REFERENCES…………………………………………………………………………….18 SECTION NINE DAHL-CHASE DIAGNOSTIC SERVICES NON-GYN CYTOLOGY FINE NEEDLE ASPIRATION PHYSICIAN GUIDE
GENERAL STATEMENT Fine needle aspiration biopsy (FNAB) has been demonstrated reliable in assessing neoplasms, infections, and reactive lesions of salivary gland, thyroid, lymph nodes, breast, and soft tissues. Its primary advantage is low cost, minimal morbidity, and rapid diagnosis. Acceptable target lesions include virtually any defined, palpable mass of the head and neck, breast, axilla, extremities, or subcutaneous skin. Fine needle aspiration biopsy is extremely safe for superficial lesions (intraabdominal and intrathoracic lesions carry an increased risk and should be performed under radiologic guidelines by experienced operators). The most frequent cause of a false negative diagnosis is a geographic miss of the lesion, an outcome with significantly increased frequency when inexperienced operators are performing the procedure. It is therefore imperative that FNAB should be interpreted in the context of clinical and radiologic findings, and that discordant FNAB results should be explained by repeat FNAB or another procedure. PRE-PROCEDURE CONSIDERATIONS Work up Algorithm
1. Pertinent clinical history and any relevant imaging or pathologic studies and differential
diagnostic considerations with appropriate consultations with colleagues, or the chart.
a. Thyroid scan should be performed prior to FNAB due to possible interference with
b. CT/MRI scan results are not affected by FNAB.
2. Questions the study is attempting to answer.
3. Knowledge of how to perform the procedure.
Target Lesion
1. Virtually any palpable, well-defined subcutaneous mass is an acceptable target lesion for
2. Subcutaneous lesions near vital structures such as major arteries or the pleura (as in
supraclavicular or chest wall FNAB) carry increased risk of significant complications, and should be performed by experienced operators only.
3. Ill-defined lesions such as post-radiotherapy indurations or “thickenings” of the breast
often are poor targets and frequently yield non-diagnostic results.
4. “Blind” FNAB of lesions identified radiologically, but not palpable, should not be
5. If lesion is not palpable, ask patient to help localize. Defer study if not palpable and
document that procedure was deferred and the reasons why.
Contraindications
1. Vague, ill-defined or non-palpable lesions.
2. Lesions too near pleura or vital structures to perform FNAB safely.
3. FNAB should not be performed on suspected carotid body tumors due to the possibility of
a. For patients with major coagulopathies (i.e. hemophilia, platelet counts less than
5000, or hematologic malignancies), one may wish to consider alternative diagnostic maneuvers or therapeutic correction of the coagulopathy prior to attempting FNAB. PT/PTT and a bleeding time should be evaluated in such patients.
b. FNAB may be safely performed on patients on therapeutic doses of Coumadin.
Care should be taken to apply prolonged tamponade (5-10 minutes) of the biopsy site after FNAB.
c. If the lesion is highly vascular (i.e. thyroid) or in a site (i.e. neck) that a hematoma
could be life threatening, consideration should be given to alternative diagnostic maneuvers.
Complications
1. As in phlebotomy, vasovagal reactions and fainting are by far the most common
2. Hematomas may occur, but can be avoided by adequate tamponade of the biopsy site.
Between passes and after the procedure, a gauze pad may be gently pressed against the puncture site.
3. Infections have been reported, but are exceedingly rare.
4. Improper technique for lesions of the chest wall or supraclavicular region may result in
6. Theoretical concerns about tumor implantation have not been born out in practice with
use of fine gauge needles. The incidence of tumor seeding is low, approximately 0.005%. However, it may be prudent, whenever feasible to include the needle track in subsequent excision of a malignancy.
1. A pertinent clinical history should be obtained and a directed physical examination is
2. FNAB of palpable subcutaneous masses is of similar risk to phlebotomy, and therefore
3. It is advisable to discuss the procedure including potential complications with the patient
or legal guardian, and to document that verbal consent was obtained.
4. For FNAB of palpable lesions near vital structures such as major arteries or the pleura,
written consent may be obtained, since these procedures carry risk of more significant complications. If one is inexperienced in FNAB technique, one may wish to refer the patient to a more experienced operator.
5. Written consent is mandatory for FNAB of radiographically detected intra-abdominal or
1. Use of anesthesia is discouraged because:
a. The wheal raised by the anesthetic often obscures the lesion, resulting in
b. Use of medication (1% Xylocaine) adds potentially life-threatening allergic
reactions to an otherwise minimally morbid procedure
c. The size of the needle used to administer the anesthetic approximates the size of
the biopsy needle and may cause more pain then the FNA itself
d. Infusion of anesthetic agent may cause degeneration and loss of cellular
2. Anesthesia is often required in a few specific situations.
a. Extremely painful lesions (e.g. infectious lymphadenitis, neoplasms with perineural
b. Breast lesions in which the areola must be traversed by the needle.
e. Extraordinarily anxious patients, with easily palpable target lesions
PROCEDURE Materials
1. Exam table or chair that can be placed into Trendeleburg position
4. 23, 25, or 27 gauge needles, 1-1.5” depending on depth of lesion/mass. Longer syringes
11. Spray fixative or 95% ETOH in screw top containers
13. Flow cytometry fixative (for lymph nodes) may be obtained from DCPA.
14. 1% or 2% Xylocaine and tuberculin syringes for anesthesia as needed
15. Culture swabs or transport medium, sterile containers (for suspected infectious lesions)
16. Other ancillary studies – If other ancillary studies are anticipated such as cytogenetics,
electron microscopy or molecular DNA tests, please have the necessary equipment
Position
1. The biopsy may be performed with the patient lying or sitting. If sitting, the setting should
allow rapid placement of the patient into Trendelenburg should a vasovagal reaction occur.
2. The patient should be in a position that allows the aspirator to be in a logical, comfortable
position. If the operator is in an awkward position while performing the biopsy, it is unlikely diagnostic material will be obtained.
3. The lesion should be carefully examined prior to the biopsy to ensure it can be
adequately immobilized by the index and middle fingers of the nondominant hand. Ensuring the stabilization of the mass and approaching the biopsy in a comfortable, organized manner may take longer than the biopsy itself, but is well worth the effort given the increased accuracy of needle placement and quality of material obtained.
Technique
The object of FNAB is to use the tip of the needle as a microscalpel to core out minute tissue fragments, with minimal contamination by peripheral blood. Suction does not contribute to the procurement of cells; rather its function is to hold the sample in the needle. Indeed, excellent samples can be obtained with no suction applied. It is highly desirable to keep the entire specimen confined to the needle alone since a sample that is drawn into the syringe usually never makes it out to the slide, and is wasted.
1. Label 5-10 slides and containers to be used in the room with patient’s full name, date of
birth or MR# and biopsy site after the patient is in the room and after you have determined the procedure will be performed.
2. Antiseptic Preparation: Wash hands, put on gloves, clean skin with alcohol swab (use
Betadine near joints or other sterile spaces that could be accidentally entered). After excluding possible allergies, anesthetize skin if indicated.
a. Attach needle to syringe with plunger and place in syringe holder (Draw 1 ml into
syringe before aspiration to facilitate expression of cells onto a slide).
b. Immobilize the lesion with index and middle fingers of the nondominant hand.
c. Introduce needle attached to syringe and syringe holder into the lesion. (Do not
apply negative pressure). The thumb or index finger of nondominant hand can be used to stabilize the syringe as the needle is directed into the lesion.
d. With needle in the lesion, apply 1-2cc of negative pressure.
e. Perform biopsy using fine, back and forth oscillations of the needle (similar to an
electric sewing machine) for approximately 10 seconds, 10-15 cycles of the needle, or until blood appears in the hub of the needle. Stop needle oscillations. Important: Always stop biopsy when blood appears in the hub of the needle. Specimen in the syringe usually clots or dries, and is lost for diagnostic purposes. Excursions should be in the same horizontal and vertical planes; do not “fan” the axis of the needle as this causes increased bleeding.
f. Release suction with needle in lesion, to avoid sucking the specimen into the
5. Perform smears (see Part V Smears and figure 1).
6. Rinse needle into CytoRich Red fixative solution by drawing 1-2ml of CytoRich Red
through needle into syringe and express all fluid back into CytoRich Red container. Repeat rinse 2-3 times.
7. Repeat technique for total of 3 or more biopsies.
Follow steps above except use a needle alone or needle attached to a band of a syringe without a plunger (band useful if lesion ends up being cystic). This method decreases the amount of blood in the specimen and affords greater tactile sensation of the lesion through the needle. Holding the hub in a “pencil” grip, the aspirator inserts the needle into the lesion/mass and moves the needle tip within the lesion/mass in an up-and-down motion in 3- to 5-mm strokes.
9. Discard any unused slides, containers, or printed labels. Dispose of needles
appropriately, clean equipment and room as necessary.
Common Errors in Technique
1. Failure to adequately stabilize the mass, resulting in errant needle placement
(geographic miss) and false negative biopsy.
2. Use of too large needle (use 23 gauge or smaller to avoid excessive contamination by
3. Operator aspirates instead of biopsies (i.e. tries to “suck out” cells). Use staccato, sewing machine-like motion to core out tissue fragments. Slow, saw-like motion also results in poor cell yield.
4. Aspirator continues to draw sample into syringe even after sample appears in hub of
needle. Sample will clot and air dry inside syringe. Always stop when blood appears in the hub.
5. Needle is removed from patient with suction on. Specimen is drawn into the syringe,
dried, clotted, and lost for further evaluation.
6. Operator rinses entire specimen into CytoRich Red solution. The best diagnostic sample is obtained on smeared, alcohol-fixed material. CytoRich Red solution salvages specimens caught in the syringe; however, CytoRich Red preparations are less than adequate for evaluation of most lesions.
a. Multiple passes ensure that different areas of the lesion are sampled.
b. Multiple passes ensure against geographic misses.
c. Three or more passes are optimal for all lesions. Large lesions may have
extensive necrosis, fibrous stroma and often yield scantly cellular specimens.
8. Operator drains cyst without sampling cyst wall. Cyst fluid, although abundant, seldom
contains diagnostic cells. Always perform additional passes of the cyst bed, or any residual mass.
Excellent samples can be destroyed by smears that are poorly fixed or too thick, hence good smear technique is as important as good biopsy technique. Bloody specimens must be quickly and properly handled since blood impedes fixation or clots in the needle. Technique(see Figure 1)
1. Remove needle and draw air into the syringe, replace needle
2. Place 3-4mm droplet on slide, 1cm from frosted end
a. If more sample is available, prepare multiple slides, particularly if the specimen is
b. Use of a large droplet (greater than 5mm of sample) is likely to result in a thick,
3. With nondominant hand, pinch slide between thumb and forefinger with remaining three
4. With dominant hand, lay spreader slide perpendicular to specimen slide. Observe
5. With no pressure, glide spreader slide down the length of specimen slide and instantly fix
within 3 seconds) smeared slide. (You may wish to have an assistant ready with spray fixative).
6. Spread remaining slides with spreader slide and fix as quickly as possible.
7. Examine smeared, fixed slides for white particles indicative that diagnostic material is
present on the slide. Smears that appear to consist of blood only are likely to be nondiagnostic.
Common Errors in Smearing
1. Too much specimen placed on slide. Specimen droplet should not exceed 3-4mm in
diameter and should be placed 1cm from frosted end of the slide. For cysts and very bloody specimens, perform two or three smears and rinse the remainder into CytoRich Red solution. CytoRich Red solution will lyse some of the red blood cells and the laboratory can attempt to salvage the sample.
2. Operator waits too long to fix slides. Air drying completely destroys cell morphology.
Once a smear is prepared, it must be fixed immediately.
3. Excessive pressure in smearing the specimen will result in crush artifact and
4. Operator puts smeared slides into CytoRich Red fixative solution. CytoRich Red solution
is not an adequate fixative for smears. Use only spray fixative or 95% ethanol in screw top containers.
5. Operator fails to smear slides. Specimens that are not smeared are too thick to permit
6. Operator submits slides that are not labeled with patient’s name, date of birth or MR#,
and source of specimen. Unlabeled slides cannot be accepted by laboratory for interpretation.
7. Operator rinses entire specimen into CytoRich Red solution. The best diagnostic sample
is obtained on smeared, alcohol-fixed material. CytoRich Red solution salvages specimens caught in the syringe; however, CytoRich Red preparations are less than adequate for evaluation for most lesions.
Lymph Nodes
All lymph nodes whether suspected to be reactive or lymphoma, should have material obtained for flow cytometric analysis of lymphoid markers. This should be procured in addition to standard smear preparations.
After obtaining smear specimens, perform one or two additional passes, and rinse the entire specimen into flow cytometry medium (RPMI). Send specimen to flow cytometry lab. Please call 941-8200 if there are questions. Suspected Infections
Cultures can be successfully obtained from FNAB material.
1. If pus is obtained, prepare 1-2 smears for cytology in the standard smear fashion. Save
the remainder of the specimen in the syringe. Remove the needle and replace with original plastic syringe cap. Label syringe/container and smear with full name, date of birth or MR#, and source, and forward to Microbiology. Prioritize the type of cultures needed, as specimen quantity may be insufficient for all assays.
2. If no fluid specimen is obtained, express a drop or two of specimen from the needle onto
a sterile culture swab. Place swab into transport medium. Label with full name, date of birth or MR#, and source and send to Microbiology. This type of preparation is unsuitable for mycobacterial cultures or gram stains. Alternatively, rinse the needle into sterile nonbacteriostatic saline in a sterile tube. This is less optimal due to possible contamination by skin flora on the outside of the needle. (Thioglycolate broth may be used if available instead of sterile saline).
3. Air dried smears can be sent to Microbiology for AFB/Gram stains.
1. Whether a benign cyst or a cavitated, necrotic malignancy, cyst fluid does not generally
2. If fluid is obtained when suction is applied to the needle, do not perform the finely
oscillating biopsy technique, rather, leave the needle stationary and apply enough suction to completely drain the cyst.
3. If the syringe fills prior to total decompression of the cyst, perform multiple sticks until all
a. If a residual mass persists, perform one or two FNAB using the standard
b. If no mass persists, perform one or two “blind” FNAB of the cyst bed in an attempt
5. Make one or two slides from the cyst fluid, and place the remainder directly into CytoRich
Red solution. FNAB of any residual mass or “blind” sticks of the cyst bed should be smeared in the method described in Part V Smears.
Site Specific Considerations 1. Breast
To determine the position that best exposes the breast lesion/mass, palpate the lesion/mass while the patient is in a sitting position, and again while the patient is supine. Having the patient lie down with the ipsilateral arm raised above the head facilitates palpation of the lesion/mass. During aspiration, the lesion/mass should be stabilized between two fingers of the nondominant hand of the aspirator. The size of the lesion/mass should determine which two fingers to use. If the lesion/mass is larger than 2 cm, it can be held between the thumb and the index finger, if feasible. If the lesion/mass is smaller than 2 cm, stabilize it between the index and third (middle) fingers. Aspiration through the areola should be avoided, if possible. Lesions/masses under the nipple or areola can usually be aspirated by pushing the nodule away from the nipple and aspirating through the adjacent skin avoiding the areola if possible. Care should be taken not to accidentally pierce the pleura when aspirating a deep-seated breast lesion/mass. If a breast aspiration results in a clear fluid and the mass disappears, the fluid may be discarded. Bloody or cloudy fluid may yield cells that may be diagnostic, but clear fluid generally does not yield significant cells and could indicate a simple cyst, which may be curative as well as diagnostic. If a mass persists after evacuation of the cyst, reaspirate the residual mass.
2. Axillary Lesions/Masses
Usually, axillary lesions/masses are lymph nodes and they are often difficult to immobilize. Aspiration can be done while the patient is sitting up or lying down. Sometimes abducting the patient’s arm with an assistant supporting it helps in palpation of the lesion/mass. If no assistant is available, the patient can rest the arm on the aspirator’s shoulder. The aspirator can use his or her index and middle fingers to immobilize the lesion/mass by reaching above the lesion/mass and pulling it down while fixing it against the chest wall. To facilitate aspiration, use the thumb to further immobilize the lesion/mass. The aspirator might prefer to sit slightly lower than the patient. To prevent accidental piercing of the pleura, especially in thin patients, the needle should enter the lesion/mass almost parallel to the chest wall
3. Thyroid
The patient may be seated or supine; a pillow placed under the patient’s shoulders can extend the neck and increase exposure of the gland. There are differing views on the optimum position of the aspirator relative to the patient. Some suggest standing above the head of a supine patient, while others advise that the aspirator be positioned at either side of the patient. While each position has its merits, the stance in which the aspirator feels most comfortable palpating and localizing the lesion/mass is most likely to yield adequate material. The aspirator should stabilize the nodule against deeper tissue using the index and middle fingers or thumb and forefinger of the aspirator’s nondominant hand. It is useful to have the patient swallow before the biopsy to reduce the patient’s
urge to do so during the procedure. The aspirator stretches the overlying skin between the fingers before inserting the needle to reduce the patient’s pain. The needle is inserted perpendicular to the skin and into the mass. Minimal (5 ml) or no suction may be applied to reduce bleeding. Instruct the patient not to swallow once the needle is inserted in the lesion/mass. In the case of a midline lesion/mass, especially those smaller than 2 cm, the trachea can be entered accidentally. If that occurs, the patient might cough. Instruct the patient to signal if a cough is imminent so that the aspiration can be terminated. Apply local pressure as soon as the needle is withdrawn. This reduces the risk of a hematoma.
4. Subcutaneous Lesions/Masses.
Lesions/masses less than 1 cm can be immobilize by advancing the nodule under the skin until it will not move any further. Without lifting the fingers, the overlying skin is retracted and the aspiration is performed in front of the fingers. Alternatively, if the nodule is small and freely movable, it may be grasped and lifted between the thumb and fingertips of the aspirator’s nondominant hand during aspiration. In the case of a plaque-like recurrent tumor near scars, the aspiration is done by inserting the needle (26-g or narrower) parallel to the skin surface so as to take a specimen of the plaque and not the underlying adipose tissue.
5. Fat Pad Aspirations
Amyloid is a pathologic hyaline proteinaceous substance, deposited between cells in various tissue and organs of the body in a wide variety of clinical settings. Amyloid is distinguished from other hyaline deposits with the histochemical Congo red stain that stains amyloid salmon pink and demonstrates green birefringence upon polarization. Amyloidosis is a group of diseases that have in common the deposition of similar appearing proteins. Examination of abdominal fat pad aspirates stained with Congo red can be used for the diagnosis of systemic amyloidosis. This test is specific but its sensitivity is low and inadequacy is high.
The general guidelines for fine needle aspiration apply to the abdominal fat pad aspirate with some special considerations. Perform 3-5 passes of the abdominal wall fat pad usually inferior and lateral to the umbilicus. A larger needle (up to 18 or 19 gauge) rather than the usual 23 to 27gauge needle may be used for better sampling of the vessels, which may contain the deposits of amyloid. There should be visible fragments of adipose tissue on air-dried smears for an adequate specimen. Material for a cell block may also be helpful. The laboratory stains the slides and/or cell block with the Congo red stain and reports the results with an adequacy statement and indicates whether the findings are non-diagnostic, positive or negative. Due to the low sensitivity of the test, a negative result does not exclude the diagnosis of amyloidosis. Clinical correlation is advised with follow-up as clinically indicated.
1. If significant swelling, pain, fever or respiratory distress occurs after the FNAB, the
2. For small amount of pain, minor analgesics such as acetaminophen are adequate as
3. There are no restrictions as to bathing, exercise, medications, etc
4. After salivary gland aspiration, the patient may experience the taste of blood following the
procedure as well as local discomfort during meals for a couple of days.
1. The requisition form should include the specific site where lesion is located. “Breast” or
“Neck” is not specific enough. Examples include:
a. Left breast at 6 o’clock, 3cm from left nipple b. Right lateral neck, 1cm from angle of jaw c. Left upper thyroid lobe
2. All slides must be labeled with the patient’s full name, DOB or MR#, and source of
3. Basic patient demographics and physician’s name should be included on a non-gyn
cytology requisition including persons or department to be copied in the report
4. Pertinent patient history including any history of radiation, chemotherapy, recent trauma
or surgery is essential, since cellular changes related to these procedures may mimic malignancy on cytology.
5. State clinical and radiographic impressions as to benign, indeterminate or malignant, the
size, duration and nature of the mass (solid, cystic, mixed) number of passes, quantity and gross appearance of aspirate if pertinent. This aids us in assessing if the cytologic findings are representative of the clinical lesions, and hence, if the mass truly has been sampled.
6. Any history of prior malignancy. This is useful so we can compare the morphology of the
prior tumor to determine if the new mass is metastatic or primary.
1. If the specimen is received in the Cytology Lab prior to 11 a.m., the routine result will be
2. Specimens received later can be processed and interpreted the same day in emergency
situations. The Cytology Lab should be notified by telephone (941-8200) as early as possible in the day so that arrangements can be made to rush the specimen.
If you experience difficulty in obtaining adequate samples or have any questions, our pathologists are pleased to speak with you. We can arrange to observe your technique and give suggestions about how to improve your diagnostic yield for FNAB. If you have any further questions regarding FNAB, please call 941-8200 from 8:00 a.m. to 5:00p.m. Monday through Friday. REFERENCES:
1) National Cancer Institute Consensus Conference. The Uniform Approach to Breast Fine Needle
Aspiration Biopsy. Developed and approved at the National Career Institute in Bethesda, Maryland. September 9-10, 1996. Diagnostic Cytopathology 1997, 16: 295-309.
2) National Committee for Clinical Laboratory Standards (NCCLS). Fine Needle Aspiration Biopsy
(FNAB) Techniques; Approved Guidelines (NCCLS Document GP20-A2). NCCLS, Vol. 23 No. 27, 2003.
3) Papanicolaou Society of Cytopathology. Guidelines of Papanicolaou Society of Cytopathology
forFine Needle Aspiration Procedure and Reporting. Modern Pathology 1987; 10(7): 739.
4) Non-Gynecological Cytology Practice Guidelines. American Society of Cytopathology.
2004.5)Robbins & Cotran. Pathologic Basis of Disease, 7th Edition. p 258-9.
Written by: Teri Cooper, M.D. (1997) Revised by: Holly McDaniel, M.D. (2000), Carol Trask, M.D. (2006 and 2011) SECTION NINE DAHL-CHASE DIAGNOSTIC SERVICES NON-GYN CYTOLOGY DETAILED COLLECTION AND SUBMISSION REQUIREMENTS
Bladder Wash Principle
Cytologic studies are performed on Bladder Wash sediment to detect bladder cancer that may be undetectable by cystoscopy Collection and Submission
Bladder washings are obtained by cystoscopy and should be fixed immediately by adding 70 ml of specimen to 30ml of CytoRich Red solution. The specimen must be labeled with the full patient's name, second identifier (DOB or MR #), and source and sent to Dahl-Chase Diagnostic Services accompanied by a completed Non-Gyn Cytology Request Form noting any pertinent clinical information such as history of malignancy. Body Fluids Principle
Cytology studies are performed on Body Fluids (Pleural, Pericardial, Abdominal, Cul-de-sac, Pelvic washes and Synovial fluids) to detect metastatic carcinoma, mesothelioma, rheumatoid disease and inflammatory conditions. Collection and Submission Pleural, pericardial, abdominal and Synovial fluids are collected by needle aspiration.
Agitate collection container and pour 60 mls of fluid into a pre-filled 60 mls CytoRich Red container. If less than 50 mls of fluid is available, make a 50:50 mix of specimen to CytoRich Red.
If additional fluid remains, pour 60 mls into a sterile container with a tight lid and send unfixed (refrigerated).
If additional fluid remains, send up to two more pre-filled CytoRich Red containers as above.
Label all containers with the patient's full name, second identifier (DOB or MR#), and source
Any remaining fluid should be kept refrigerated at the hospital laboratory for up to 3 days.
Cul-de-sac fluids and abdominal washes are usually collected at laparoscopy. If the specimen has been obtained using saline, then it needs to be fixed with CytoRich Red solution as described above. Heparin may be added (5 units/ml of body fluid) if the specimen is clotting. If a small amount of fluid (<5ml) is collected or there will be a delay in transporting, the fluid should be added to an equal amount of CytoRich Red solution. The specimen must be labeled with the patients full name, second identifier (DOB or MR #), and source and submitted to Dahl-Chase Diagnostic Services accompanied by a completed Non- Gyn Cytology Request Form noting any pertinent clinical information such as history of malignancy. Principle
Cytology studies are performed on bronchoscopy specimens (bronchial brush, bronchial trap and bronchial wash) to detect lung cancer. Herpes virus, Cytomegatlovirus(CMV), Aspergillus and Pneumocystis among others may also be detected. Cytology studies are performed on broncho alveolar lavage to detect vegetable cells, microorganisms, ferruginous bodies, lipid-laden macrophages, and hemosiderin-laden macrophages. Cytology studies are performed on Wang needle aspirations of the trachea to assess mediastinal disease.
Collection and Submission Bronchial brushings are obtained from a specific area of the bronchial tree during bronchoscopy. The brush from the procedure should be rapidly rotated on the surface of a slide and the smear fixed immediately with 95% alcohol or spray fixative. Bronchial washings are obtained from a specific area of the bronchial tree by instilling 10ml of normal saline in small portions and re-aspirating the material with suction. The material collected should be fixed with equal parts of CytoRich Red solution. Bronchial traps are the mucus traps that are used to suction secretions during the bronchoscopy procedure. Material from any area of the lung that was sampled would be present in the trap, which should be fixed with equal parts of CytoRich Red solution. Broncho alveolar lavage specimens are obtained when the bronchoscope is advanced into a bronchial segment until it gently occludes the lumen. Aliquots of 20-60 ml of sterile normal saline are infused and re-aspirated and collected in a suction trap. If this is part of a bronchoscopy procedure, the specimen may be submitted with the other material collected. Wang from bronchoscopy is obtained by needle aspirations through the trachea wall into the mediastinum with the use of a Wang needle. The specimen is aspirated into the needle and the needle is withdrawn and rinsed in CytoRich Red solution. Alternatively, smears may be made by smearing the aspirated material between two glass slides and immediately fix in 95% alcohol or spray fixative.
All specimens and slides must be labeled with patient's full name, second identifier (DOB or MR #), and source and submitted to Dahl-Chase Diagnostic Services with a completed Non-Gyn Requisition Form noting any pertinent clinical information. All of the specimens that are collected may be submitted with one requisition. Specimens for Special Stains
Special stains may be performed to highlight the presence of microorganisms, lipid and iron. Special stain slides are made in addition to the routine cytology material. Broncho alveolar lavage is the preferred specimen for all stains, but they may be performed on bronchial washings, bronchial traps, and bronchial brushes. Sputum is less than optimal for special stains.
Collection and Submission GMS-pneumocystis for the detection of Pneumocystis GMS-fungus for the detection of fungus including candida and Aspergillus AFB for the detection of mycobacteria Iron stain for the detection of hemosiderin-laden macrophages
These stains are performed when ordered on the requisition.
Fat stain for detection of lipid laden macrophages. A fresh specimen (unfixed) must be submitted for detection of lipids in specimens. The fresh specimen must be submitted in addition to the routine cytology material.
CSF and Vitreous Fluid Principle
Cytologic studies are performed on CSF and Vitreous fluid to detect metastatic carcinoma, lymphoma, leukemia, cryptococcus, and inflammation. Collection and Submission CSF is collected at lumbar puncture. At least 1ml of CSF should be sent fresh, refrigerated to Dahl-Chase. This specimen should be sent without delay, especially for suspicion of leukemia and lymphoma. The specimen must be labeled with the patient's full name, second identifier, (DOB or MR #), and source and submitted to Dahl-Chase Diagnostic Services accompanied by a completed Non-Gyn Cytology Request Form noting any pertinent clinical information such as history of malignancy or lymphoma. Vitreous fluid is obtained by aspirate or washing. At least 1ml of vitreous fluid should be sent fresh, refrigerated to Dahl-Chase. The specimen must be labeled with the patient's full name, second identifier (DOB or MR#), and source and submitted to Dahl-Chase Diagnostic Services accompanied by a completed Non-Gyn Cytology Request Form, noting any pertinent clinical information. Specimens for special stains GMS-Fungus for detection of fungus including cryptococcus. Gastrointestinal Tract Brushings Principle
Cytologic studies are performed on the gastrointestinal tract to detect or rule out cancer. Esophageal brushings may also detect Herpes or Candida. Collection and Submission
Specimens from the GI tract are obtained by endoscopy. A brushing from a visible lesion is obtained prior to the biopsy. The brush should be rapidly rotated on the surface of the slide and the smear fixed immediately in 95% ethanol or spray fixative to avoid air-drying of the specimen. The slides must be labeled with the patient's full name, second identifier (DOB or MR #), and source on the frosted end with a #2 lead pencil. The slides are submitted to Dahl- Chase Diagnostic Services accompanied by a completed Non-Gyn Cytology Request form noting any pertinent clinical information. Nipple Discharge Principle
Cytology studies are performed on nipple secretions to detect breast carcinoma, or papilloma. Collection and Submission
Gently strip subareolar area and nipple with thumb and forefinger. When secretion occurs, allow a pea-sized drop to accumulate. Apply a glass slide directly to the nipple and secretion. Fix the slide immediately with spray fixative or 95% ethanol to avoid air-drying. The slide must be labeled with the patient's full name, second identifier (DOB or MR #), and source and submitted to Dahl-Chase Diagnostic Services accompanied by a completed Non-Gyn Cytology Request Form noting any pertinent clinical information. Principle
Cytologic studies are performed on sputum specimens to detect lung cancer and respiratory infections.
Collection and Submission
The patient should expectorate early morning sputum directly into a container of CytoRich Red solution (saliva is of no diagnostic use). Morning specimens resulting from overnight accumulation of secretions yield the best diagnostic results. Three specimens on three successive days should be collected to ensure a maximum of diagnostic accuracy. The sputum specimen must be labeled with the patient’s full name, second identifier (DOB or MR#), and source and date of collection and submitted to Dahl-Chase Diagnostic Services accompanied by a completed Non-Gyn Cytology Request Form noting any pertinent clinical information. Tzanck Prep for Herpes
Principle
Cytologic studies are performed on Tzanck preparations to detect the presence of cells that are infected with Herpes virus.
Collections and Submission
A suspected lesion should have an intact vesicle to be sampled. Open the vesicle, discarding the top. Fluid in the vesicle may be used for viral culture, otherwise discard the fluid. Scrape the base of the vesicle with a scalpel blade. Try to avoid bleeding. Smear the material collected on the scalpel blade onto a slide and immediately fix the specimen with spray fixative or 95% ethanol before air-drying occurs. The slides must be labeled with the patient's full name, second identifier (DOB or MR #), and source and submitted to Dahl-Chase Diagnostic Services accompanied by a completed Non-Gyn Cytology Request Form noting any pertinent clinical information. Urine Principle
Cytology studies are performed on urine sediment to detect bladder cancer. CMV may also be detected.
Collection and Submission
Collect random voided urine (not first morning) in a clean, wide-mouth jar and add equal amounts of urine to CytoRich Red solution. For cytologic evaluation of the bladder, three samples of urine obtained on consecutive days are recommended.
• Fresh, unfixed urine specimens must be received in the lab the same day as collected
• Refrigerated urine specimens must be fixed with CytoRich Red within 6 hours of collection.
For newborns, add the small amount of urine collected to the same container of CytoRich Red solution over an 8-16 hour period.
Because urine specimens may be obtained with a catheter, it is extremely important to note the method of collection as either voided or catheterized on the requisition and the container.
The specimen must be labeled with the patient's full name, second identifier (DOB or MR #), and source and date of collection and submitted to Dahl-Chase Diagnostic Services accompanied by a completed Non-Gyn Request Form noting any pertinent clinical information.
Guidelines for Shipping Cytology Specimens
1. Pap smear slides or Non-Gyn slides must be submitted in cardboard holders that are
2. All slides must be labeled on the frosted end in #2 pencil with patient's full name, second
identifier (DOB or MR#), and source, labeling the slide holder is not sufficient as each slide must be labeled.
3. Non-Gyn specimens must be submitted in leak proof containers. The containers of
CytoRich Red solution that are provided for specimen fixation and transport are leak proof.
4. All specimens must additionally be placed in a zip lock biohazard bag before being sent
5. Do not submit large volume fluids in any large containers such as large glass vacuum
bottles or pleuravac containers. Shipping large containers like these can be hazardous to handle.
1. Specimens with high mucus content such as sputum and bronchoscopy specimens may
be held for 24-48 hours without fixative if they are refrigerated. Mucus coats cell, protecting them from degeneration.
2. Specimens with a high protein content such as body fluids may be held for up to 72
hours without fixation if they are refrigerated. The protein-rich fluid in which the cells are bathed act as tissue culture medium in preserving cellular morphology.
3. Specimens with low mucus or protein content such as urine must be fixed immediately.
Even a 1-2 hour delay will cause cellular degeneration because the fluid medium in which the cells are bathed contains enzymatic agents capable of causing cell degeneration. Fresh unfixed specimens with suspicion of leukemia or lymphoma must be submitted without delay.
4. Specimens with low pH such as gastric material must be fixed within minutes of
collection to prevent cellular destruction by hydrochloric acid.
5. Smears that are made for cytology must be fixed immediately.
All needed materials may be ordered through Dahl-Chase Purchasing 941-8202 or 1-800-464-2332.
SECTION NINE DAHL-CHASE DIAGNOSTIC SERVICES NON-GYN CYTOLOGY ANAL SCREENING PROTOCOL (ANAL PAP AND ANAL HPV) Principle
The “Anal Pap” is a screening tool used in at-risk populations to identify individuals who have premalignant cytologic changes in their anal epithelium. Procedure
1. Moisten the Dacron swab with water, not lubricant.
2. Insert Dacron swab* approximately 1.5 to 2 inches into the anal canal.
**It is important to use Dacron and not a cotton swab, as cells tend to cling to cotton and do not release easily into cytology collection fluid.
3. Once inserted deep enough into the anus (necessary in order to collect both rectal
columnar and anal squamous cells), the swab should be pulled out, applying some pressure to the wall of the anus, rotating the swab in a spiral motion along the way.
4. The collection device should be thoroughly rinsed and swirled in the SurePath vial. After
rinsing, the collection device may be discarded.
5. Place the cap on the vial and tighten.
6. Place the SurePath vial in a plastic biohazard bag and use zip lock to seal. Insert
completed Non-Gyn Cytology Request Form in the outside pocket.
Human Papilloma Virus (HPV) Testing may also be ordered, in addition to routine cytology screening. HPV Testing on anal samples has not been validated or FDA approved. Therefore, the significance of these results is uncertain. A negative result does not exclude the possibility of an infection. If you wish to have the sample tested for HPV, please indicate on the requisition. Materials and Reagents
SurePath Vial Dacron Swab - Moistened with Water Non-Gyn Cytology Request Form Biohazard Bag Reference: ARUP Laboratories, 500 Chipeta Way, Salt Lake City, UT 84108 Written By/Date: Barbara J. Morley, CT (ASCP) May 2003
SECTION NINE DAHL-CHASE DIAGNOSTIC SERVICES NON-GYN CYTOLOGY GENERAL INFORMATION
UNACCEPTABLE SPECIMENS Unacceptable specimens include the following:
1. Unlabeled or incorrectly labeled specimens: If the specimen is irretrievable, DCDS may
call the office and fax a form to the office for the provider to fill in, sign, and fax back to us. All containers and slides must be labeled with the patient's full name, second identifier (DOB or MR#), and source. Unlabeled voided urine specimens and all other retrievable specimens will be rejected and must be recollected. Any specimens that are rejected will have a report issued indicating this.
2. Specimens received in improper fixative may or may not be processed. If we are unable
to process the specimen, the physician's office will be notified. If we are able to process the specimen, a notation will be made in the quality assurance report. If the specimen is inadequate for cytologic examination, the final report will be unsatisfactory and the reason will be stated.
3. Containers which have leaked so that insufficient fluid is left to perform the test or slides
which have broken into many pieces which cannot be glued together will be rejected: The office will be called to collect a new specimen and a report will be issued indicating that the specimen was not processed
4. Specimens that are exposed to extreme temperatures (i.e. freezing or boiling) may be
unacceptable and the office will be notified to recollect.
5. Specimens in which the source on the container does not agree with the source on the
requisition: DCDS may call the office and fax a form to the office for the responsible person to fill in, sign, and fax back to us.
6. An appropriate clinical diagnosis or symptoms is required in order to process any non-
gyn cytology specimen. Any specimens received without this information will be held until a clinical indication is obtained from the office.
7. Specimens from unauthorized sources (without appropriate credentials according to state
and local requirements) will not be accepted and specimens that lack information required for testing, such as source and provider, will be resolved by fax-back prior to processing.
The average turn around time for non-gyn cytology specimens is 24-48 hours from the date of receipt of the specimen. If extra stains are needed or if a cell block is warranted, the turn around time may be extended by another 24 hours. DAYS AND HOURS OF OPERATION
The cytology department is staffed for specimen drop-off Monday through Friday from 7:00 am-10:30 pm. For rapid results on weekends and after 5:00 pm Monday through Friday, the on-call pathologist needs to be paged by calling 973-7000 and asking to have the on-call pathologist return your call.
1. Name of the teacher :. Dr. Jinu Devi Rajkumari 2. Department : 3. Designation: 4. Date of Birth : 5. Date of joining in Cotton College : 1st September, 2003 6. Academic qualification : M.Sc., Ph.D. 7. Area of Specialisation : Cytogenetics & Plant Breeding 8. Research Project : Minor Project. Title of the Project : Studies on production potential
Information provided is intended to inform clients of expected procedures and outcomes. However, not al patients, proceduresor surgeons are the same, and information may not be applicable to al procedures. PIAC reserves the right to vary the waythat a procedure is performed or which technique is used. During breast augmentation, a breast implant isplaced either under the breast tissue and
 SECTION NINE
SECTION NINE 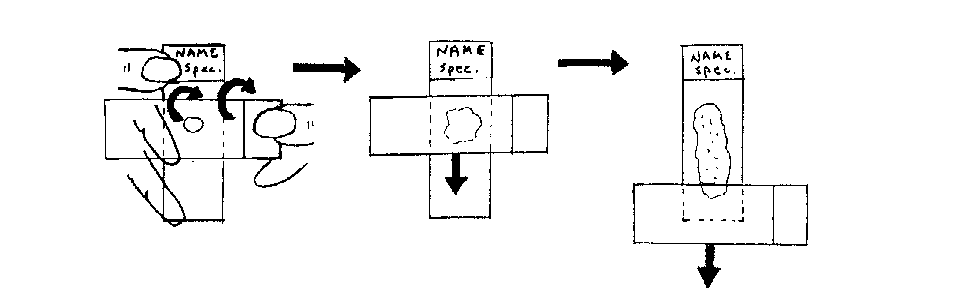 Excellent samples can be destroyed by smears that are poorly fixed or too thick, hence
Excellent samples can be destroyed by smears that are poorly fixed or too thick, hence