TOBACCO (smoke, chew, dip) ______________________ __________________________ ALCOHOL (beer, wine, hard liquor) ____________________ __________________________ CAFFEINE (colas, coffee, tea) ________________________ ___________________________ IMPAIRMENTS: Check if you have any of the following: Physical Impairment ____________ Visual Impairment ______________ Hearing Impairment __________ EXERCISE: Do you exercise regularly? ___Y ____N If Yes: Please note exercise & how often: STRESS MANAGEMENT: Do you practice stress management techniques? ___Y ____N If Yes, pls describe: DIET: Describe your typical daily food intake: Breakfast: Lunch: Supper: Any Snacks/other: 3) DOCTOR INFORMATION: Please list each Dr. from whom you seek care with address & phone number. 4) ALLERGIES: please check all that apply: ___None Known __penicillin __codeine
Note allergic reaction: ________________________________________________________________ ___________________________________________________________________________________ 5) OVER THE COUNTER (OTC) ISSUES: Please check all products used regular or occasionally. __pain reliever __ibuprofen (eg. Motrin)
__other: ___________________________________ __Nutritional/Natural Supplements: Pls identify and list products you are using: -herbs, vitamins, minerals, supplements, enzymes, others 6) MEDICAL CONDITIONS/DISEASES. Please check all that apply to you.
__heart disease
__other: _______________________________________________________________________________
7) PRESCRIPTION MEDICATION: List all prescription medication you are using (include physician samples)
____________________________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
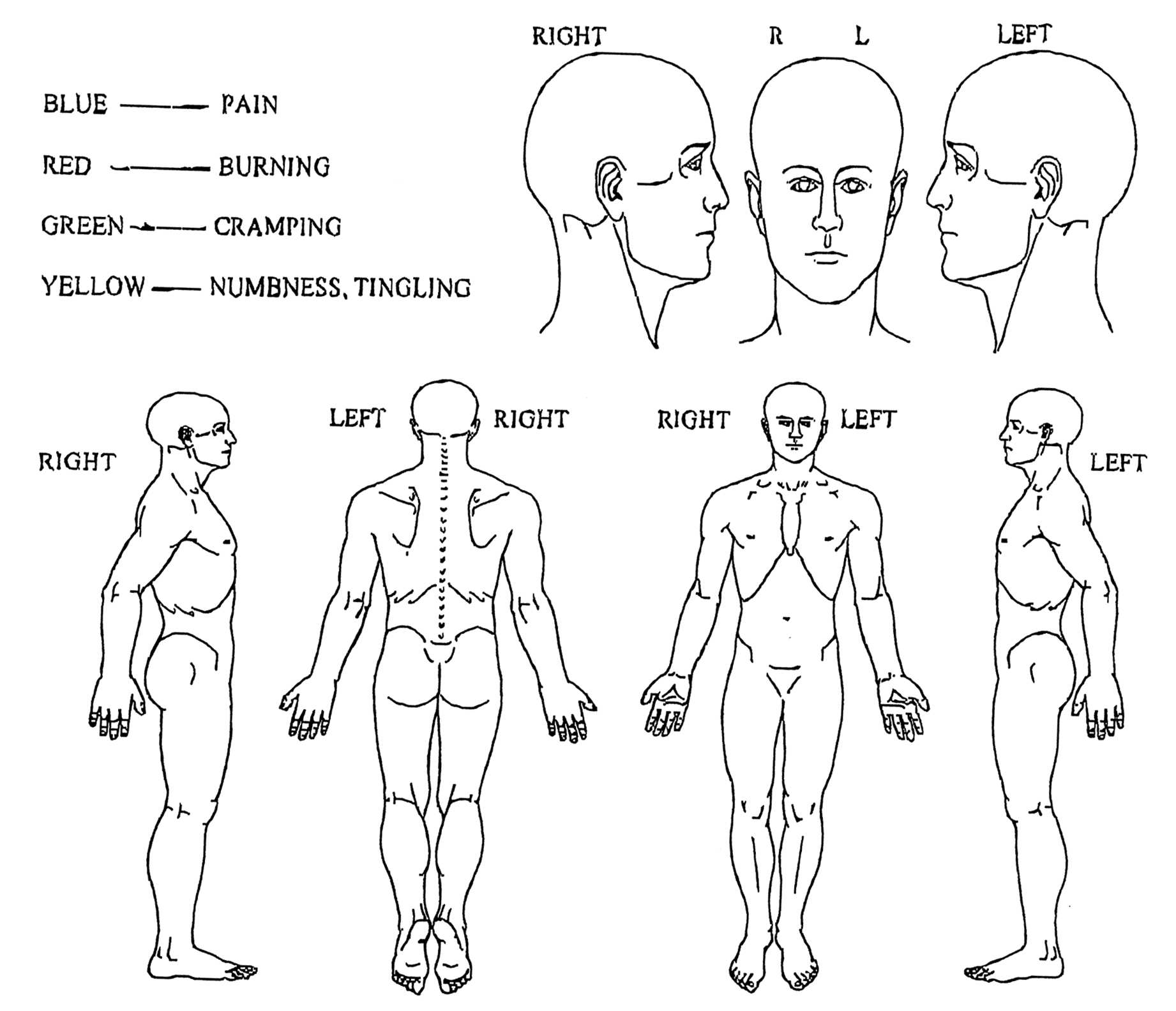
NAME__________________________________________________________DATE_________________ Circle the number that best describes your pain, 0 is NO PAIN and 10 is WORST IMAGINABLE PAIN.
Circle the number that best describes your pain at its worst during the last month.
Circle the number that best describes your pain at its least during the last month.
Circle the number that best describes your pain on average during the last month.
Circle the number that best describes your pain as it is right now.
Brothers/Sisters Please check box/boxes to indicate who has legal custody: Please furnish court documents to the school principal. Address Cell Phone # ___________Pick up rights?___ Cell Phone # ___________Pick up rights?___ Cell Phone # ___________Pick up rights?___ Has either parent had parental rights revoked? ___ Yes ___ No Which Parent? ______________ Document # ______________
Nutrition and Cancer Brown Kelp Modulates Endocrine Hormones in Female Sprague-Dawley Rats and in Human Luteinized Granulosa Cells1 Christine F. Skibola,*2 John D. Curry,*3 Catherine VandeVoort,† Alan Conley,** andMartyn T. Smith* *School of Public Health, University of California, Berkeley, California; and †California National PrimateResearch Center and **Department of Population H

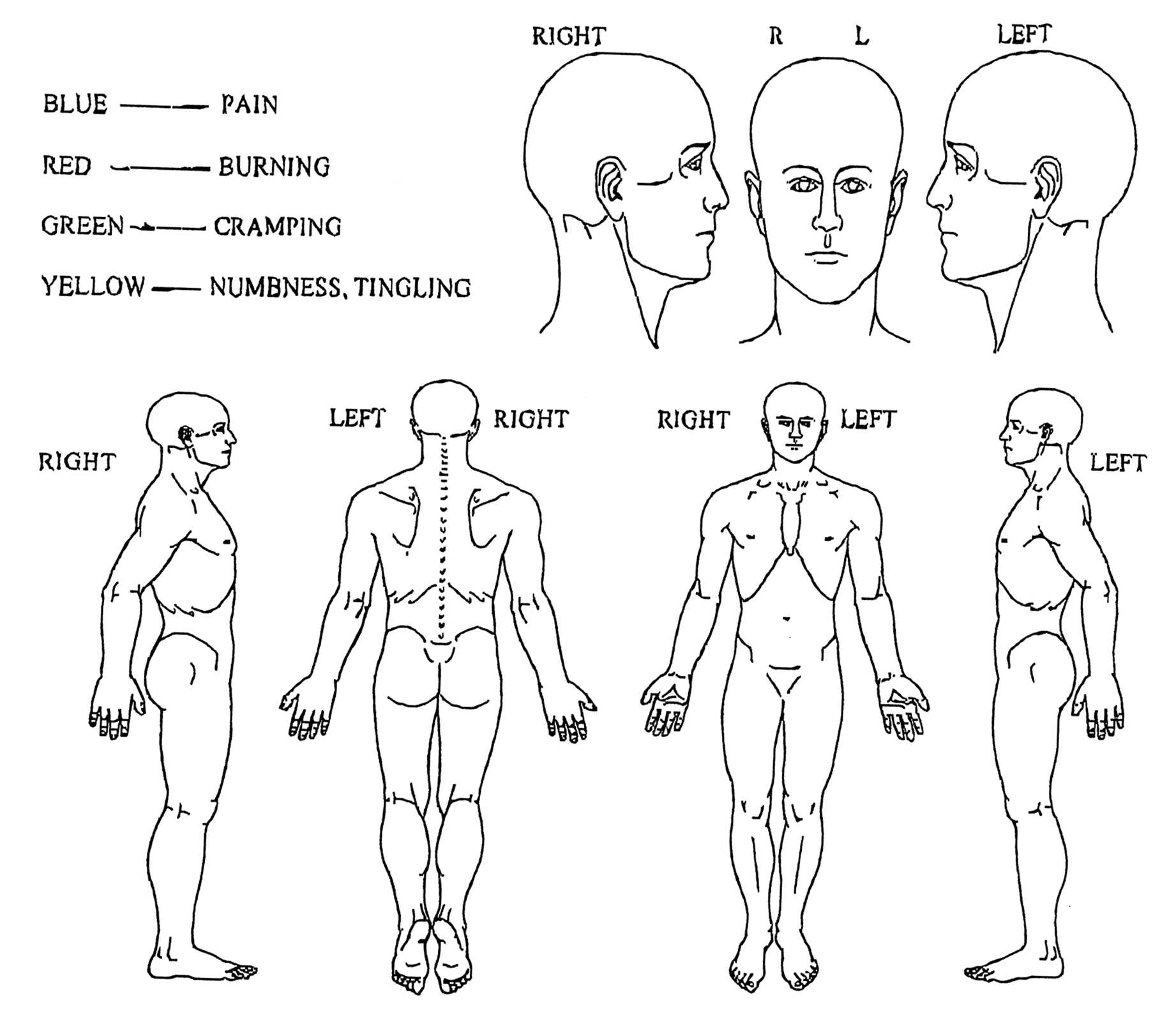
 NAME__________________________________________________________DATE_________________ Circle the number that best describes your pain, 0 is NO PAIN and 10 is WORST IMAGINABLE PAIN.
Circle the number that best describes your pain at its worst during the last month.
Circle the number that best describes your pain at its least during the last month.
Circle the number that best describes your pain on average during the last month.
Circle the number that best describes your pain as it is right now.
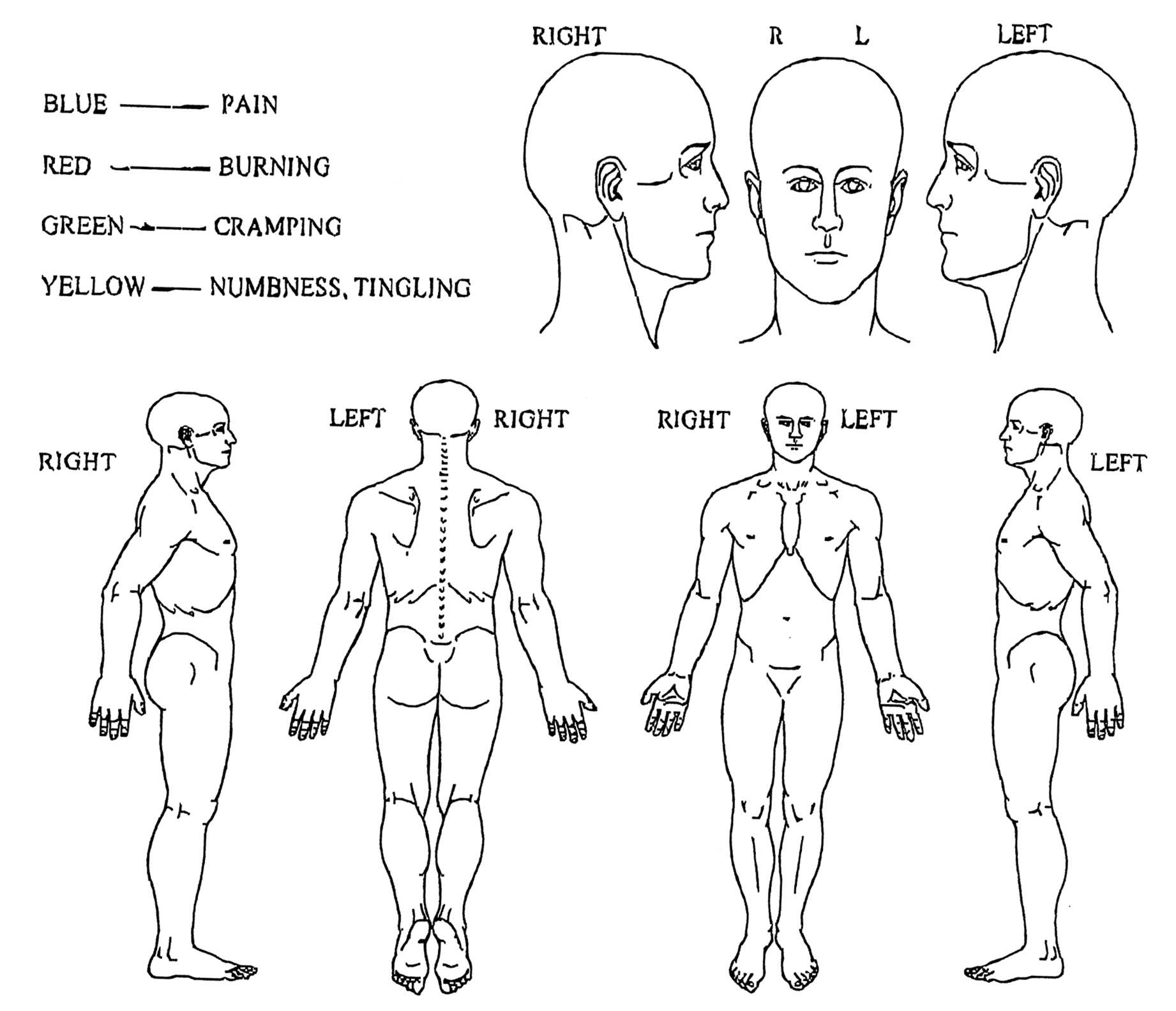
NAME__________________________________________________________DATE_________________ Circle the number that best describes your pain, 0 is NO PAIN and 10 is WORST IMAGINABLE PAIN.
Circle the number that best describes your pain at its worst during the last month.
Circle the number that best describes your pain at its least during the last month.
Circle the number that best describes your pain on average during the last month.
Circle the number that best describes your pain as it is right now.