CLINICAL OBSERVATIONS, INTERVENTIONS, AND THERAPEUTIC TRIALS
Rituximab for the treatment of refractory autoimmune hemolytic anemiain children
Marco Zecca, Bruno Nobili, Ugo Ramenghi, Silverio Perrotta, Giovanni Amendola, Pasquale Rosito, Momcilo Jankovic,Paolo Pierani, Piero De Stefano, Mario Regazzi Bonora, and Franco Locatelli
Autoimmune hemolytic anemia (AIHA) in undergone splenectomy. After complet- 8, and 10 months after rituximab infusion, children is sometimes characterized by a ing treatment, all children received intra- respectively. All 3 children received a severe course, requiring prolonged ad- venous immunoglobulin for 6 months. second course of rituximab, again achiev- ministration immunosuppressive Treatment was well tolerated. With a me- ing disease remission. Our data indicate therapy. Rituximab is able to cause selec- dian follow-up of 13 months, 13 patients that rituximab is both safe and effective in tive in vivo destruction of B lymphocytes, (87%) responded, whereas 2 patients did reducing or even abolishing hemolysis in with abrogation of antibody production. not show any improvement. Median hemo- children with AIHA and that a sustained In a prospective study, we have evaluated globin levels increased from 7.7 g/dL to a response can be achieved in the majority the use of rituximab for the treatment of 2-month posttreatment level of 11.8 g/dL of cases. Disease may recur, but a sec- AIHA resistant to conventional treatment. (P < .001). Median absolute reticulocyte ond treatment course may be successful Fifteen children with AIHA were given counts decreased from 236 to 109 ؋ 109/L in controlling the disease. (Blood. 2003; rituximab, 375 mg/m2/dose for a median (P < .01). An increase in platelet count 101:3857-3861) of 3 weekly doses. All patients had previ- was observed in patients with concomi- ously received 2 or more courses of immu- tant thrombocytopenia (Evans syndrome). nosuppressive therapy; 2 patients had Three responder patients had relapse, 7, 2003 by The American Society of Hematology Introduction
Autoimmune hemolytic anemia (AIHA) in children is usually
Rituximab is a chimeric, human, IgG1/ monoclonal anti-
characterized by a good prognosis; the disease often presents as an
body (MoAb) specific for the CD20 antigen, expressed on the
acute, self-limited illness, with good response to short-term steroid
surface of B lymphocytes. This antibody has induced rapid in
therapy in nearly 80% of patients.1 However, in some cases, AIHA
vivo depletion of both normal B lymphocytes and lymphoma
can be characterized by a chronic course and an unsatisfactory
control of hemolysis, thus requiring prolonged immunosuppressive
Its in vivo mechanisms of action include complement-
therapy. Especially in children younger than 2 years of age or in
mediated cytotoxicity, antibody-dependent cytotoxicity, inhibi-
teenagers, the clinical course of the disease may show either
tion of B-cell proliferation, and induction of apoptosis.4
resistance to steroids or dependence on high-dose steroids,2 with
Rituximab has demonstrated good clinical activity in the
subsequent development of severe side effects on growth, bone
treatment of relapsed, low-grade B-cell CD20ϩ non-Hodgkin
mineralization, and the endocrine system. The mortality rate in
lymphoma (NHL), particularly in patients with follicular NHL.5-8
these children with primary AIHA has been reported to be on the
The good therapeutic efficacy, coupled with its limited
toxicity, consisting primarily of infusion-related events, has led
Splenectomy, administration of immunosuppressive drugs such
to the recent use of this agent for the treatment of autoimmune
as azathioprine, cyclosporine A, or cyclophosphamide, or immuno-
disorders, with the aim of interfering with or, at best, abolishing
modulating agents, such as intravenous immunoglobulin, have
been used frequently, alone or in combinations, with the aim of
Preliminary results of this application appeared encourag-
reducing steroid dependence and controlling hemolysis. However,
ing9-17 and prompted us to evaluate, in a prospective multicenter
these therapies are not consistently effective and present a non-
study, the efficacy of rituximab for treatment of children
negligible risk of infectious complications due to their profound
affected by AIHA resistant to conventional immunosuppressive
therapy or requiring continuous high-dose steroid treatment.
From the Oncoematologia Pediatrica, IRCCS Policlinico San Matteo, Pavia,
Supported in part by grants from AIRC (Associazione Italiana per la Ricerca sul
Italy; Clinica Pediatrica I, Seconda Universita` degli Studi, Napoli, Italy; Clinica
Cancro), CNR (Consiglio Nazionale delle Ricerche), and IRCCS Policlinico
Pediatrica, Universita` di Torino, Ospedale Regina Margherita, Torino, Italy;
Ematologia-Oncologia Pediatrica, Ospedale di Nocera Inferiore, Italy; ClinicaPediatrica, Universita` di Bologna, Policlinico Sant’Orsola, Bologna, Italy;
Reprints: Franco Locatelli, Oncoematologia Pediatrica, IRCCS Policlinico San
Clinica Pediatrica, Universita` di Milano Bicocca, Nuovo Ospedale San
Matteo, P.le Golgi 2, I-27100 Pavia, Italy; e-mail: [email protected].
Gerardo, Monza, Italy; Clinica Pediatrica, Universita` di Ancona, Italy; and
The publication costs of this article were defrayed in part by page charge
Farmacologia Clinica, IRCCS Policlinico San Matteo, Pavia, Italy.
payment. Therefore, and solely to indicate this fact, this article is herebymarked ‘‘advertisement’’ in accordance with 18 U.S.C. section 1734.
Submitted November 25, 2002; accepted January 8, 2003. Prepublished online asBlood First Edition Paper, January 16, 2003; DOI 10.1182/blood-2002-11-3547.
2003 by The American Society of Hematology
BLOOD, 15 MAY 2003 ⅐ VOLUME 101, NUMBER 10
combination with cyclosporine A (2 cases) or with cyclosporine A and
Patients and methods
azathioprine (2 cases), at time of rituximab treatment.
After completing the treatment, all children received intravenous
Patient characteristics
substitutive therapy with a commercial immunoglobulin preparation (400mg/kg every 3 weeks for 6 months) to prevent therapy-induced
Five boys and 10 girls, with a median age at diagnosis of 2 years (range,
0.3-14 years), were prospectively enrolled in this study, approved by theinstitutional review boards of the participating centers. Written informedconsent was obtained from the parents. Data on one of these patients have
Definitions
Treatment response was defined as at least a 1.5 g/dL increase of
Nine children were affected by AIHA, and the other 6 patients had
hemoglobin concentration (Hb) together with a 50% reduction of absolute
Evans syndrome. We found no evidence of primary T- or B-lymphocyte
reticulocyte count, observed within 2 months from MoAb administration.
In all patients, a complete blood and reticulocyte count was performed
In 13 cases, warm-reactive autoantibodies of IgG type were demon-
twice weekly for the first 2 months or until a clinical response, meeting the
strated by the direct antiglobulin test (DAT), whereas in another case IgM
criteria, was achieved. Subsequently, patients were followed once weekly
cold agglutinins were present, and in another DAT remained
In 4 children a concomitant autoimmune disease was present at time of
Surface marker analysis
AIHA onset: systemic lupus erythematosus in 1, rheumatoid arthritis in 2,and vitiligo in 1. In one child, AIHA developed after allogeneic bone
The MoAbs used in this study for characterizing phenotype of circulating T and B
marrow transplantation, performed for treatment of mucopolysaccharidosis.
cells were: anti–Leu-4 (CD3), anti–Leu-3a (CD4), anti–Leu-2a (CD8), anti–
Further details on the clinical features of the patients enrolled and on
Leu-12 (CD19), anti–Leu-16 (CD20), anti-human IgM, antihuman IgG, and
pretreatment hematologic values are reported in Table 1.
antihuman IgA (Becton Dickinson, Mountain View, CA). Appropriate isotype-
All children had received 2 or more courses of immunosuppressive
matched controls were included. Phenotypic analysis of cell populations was
treatment. Eleven patients were given also a third immunosuppressive
performed by means of indirect immunofluorescence with fluorescein-
course, and splenectomy had been performed in 2 patients, in an attempt to
conjugated Fab2 goat anti-mouse or by direct immunofluorescence in 2-color
control hemolysis. Details on immunosuppressive therapy before rituximab
analysis using directly labeled antibodies on a FACScan flow cytometer (Becton
Dickinson). Results obtained from these patients were compared with those
Ten patients had received a median of 4 packed red blood cell (RBC)
observed in age-matched healthy children.19
transfusions before MoAb treatment (range, 2-11 transfusions). Four patientswere transfusion dependent at time of beginning of rituximab treatment. Data analysis and presentation Treatment with rituximab
Data were analyzed as of October 1, 2002. Results were expressed as
Rituximab (kindly provided by Roche, Milan, Italy) was administered
median and range or as absolute number and percentage, as appropriate or
intravenously at a dosage of 375 mg/m2/dose, as a 5-hour infusion. Three
children received 2 weekly doses, whereas 10 patients received 3 doses and
Normal distribution of pretreatment and posttreatment hematologic
the remaining 2 were treated with 4 doses of rituximab. Before each
values was evaluated with the Shapiro-Wilk W test. Pretreatment and
infusion, all children received premedication with methylprednisolone and
posttreatment hematologic values were compared using the Wilcoxon
matched-pairs test and the Student t test for dependent samples, as
In 2 patients, no concomitant therapy was administered, whereas the
appropriate. P Ͻ .05 was considered statistically significant and expressed
remaining 13 children were receiving steroids, alone (9 cases) or in
in detail; P from .05 to .1, even though not statistically significant, was
Table 1. Patient characteristics
Hematologic values before rituximab treatment
Evans indicates Evans syndrome; post-BMT, patient given allogeneic bone marrow transplantation for treatment of type 1 mucopolysaccharidosis; Rheum arth,
rheumatoid arthritis; SLE, systemic lupus erythematosus; —, not applicable. Table 2. Therapies administered before rituximab treatment
IV MPDN indicates intravenous methylprednisolone; oral PDN, oral prednisone; IV IgG, intravenous immunoglobulin; AZA, azathioprine; Cs-A, cyclosporine A;
CY, cyclophosphamide; —, not applicable.
shown in detail, whereas P Ͼ .1 was expressed as nonsignificant (NS). The
Figure 1A). Median pretreatment and 2-month posttreatment
SAS package (SAS Institute, Cary, NC) was used for the analysis of
absolute reticulocyte count was 236 ϫ 109/L (range, 118-750 ϫ 109/L;
mean, 320 Ϯ 175 ϫ 109/L) and 109 ϫ 109/L (range, 35-288 ϫ 109/L;mean, 109 Ϯ 67 ϫ 109/L), respectively (P Ͻ .01; Figure 1B).
In the 13 responding patients the median increase in Hb level 2
months after completion of treatment was 4 g/dL (range, 1.5-9g/dL; mean 4.2 Ϯ 2.2 g/dL), and the median decrease in absolute
The median follow-up for the 15 patients is 14 months (range, 7-28
reticulocyte count was Ϫ210 ϫ 109/L (range, Ϫ22 to Ϫ600 ϫ
months). All patients completed the therapeutic program.
109/L; mean, Ϫ217 Ϯ 200 ϫ 109/L).
DAT, positive in 14 of the 15 children before treatment, became
Treatment safety and infectious complications
negative in 6 of them (43%) at the evaluation performed 2 months
The treatment was generally well tolerated. Only 3 children
after the first MoAb infusion, whereas indirect antiglobulin test
presented moderate side effects during the infusions: fever in 2
(IAT) became negative in 2 of the 5 previously positive patients.
children and upper airway edema in the other. In all, side effects
Transfusion-dependent patients did not require any more RBC
promptly resolved with appropriate therapy (oral acetaminophen
transfusions 2 months after treatment discontinuation. The median
for the first 2 cases, and intravenous hydrocortisone plus inhalatory
time from the first dose of rituximab to the last RBC transfusion
salbutamol and budesonide for the third case).
One child developed primary varicella-zoster virus (VZV)
A raise in platelet count, concomitant with Hb increase, was
infection 2 months after rituximab administration; the infection
observed in patients with Evans syndrome; platelet number in-
resolved with antiviral therapy without sequelae.
creased from a pretreatment median value of 27 ϫ 109/L (range,4-61 ϫ 109/L; mean, 30 Ϯ 27 ϫ 109/L) to a value of 140 ϫ 109/L
Treatment response
(range, 64-150 ϫ 109/L; mean, 118 Ϯ 47 ϫ 109/L) 2 months afterstart of treatment.
On the whole, 13 of the 15 patients enrolled (87%) responded totreatment, showing at least a 1.5 g/dL increase of Hb and a morethan 50% reduction of absolute reticulocyte count. Two patients(13%), both affected by isolated AIHA with warm-reactive IgGautoantibodies, did not show any improvement after 3 doses ofrituximab and were considered as nonresponders (Figure 1A).
In responding patients, the 1.5 g/dL increase in Hb level was
observed after a median of 12 days from the first MoAb administra-tion (range, 5-72 days); the 50% reticulocyte reduction wasdetected after 21 days (range, 5-82 days; Table 3). Figure 1. Hemoglobin and absolute reticulocyte counts. Pretreatment and
Considering the whole study population, median Hb level
2-months posttreatment levels of hemoglobin (A) and absolute reticulocyte count (B),
increased from a pretreatment value of 7.7 g/dL (range, 3.5-10.0
as well as pretreatment and posttreatment mean values Ϯ SD for the whole studypopulation. The difference between pretreatment and posttreatment values is
g/dL; mean, 7.7 Ϯ 1.8 g/dL) to a 2-month posttreatment level of
statistically significant (P Ͻ .001). Small circles indicate the value for each patient;
11.8 g/dL (range, 6.0-14.2 g/dL; mean, 11.4 Ϯ 2.1 g/dL; P Ͻ .001;
large circles, median values for the entire study population.
BLOOD, 15 MAY 2003 ⅐ VOLUME 101, NUMBER 10
Table 3. Details of treatment with rituximab and results
*At least a 1.5 g/dL increase of hemoglobin. — indicates not applicable.
Figure 2A shows the raise of haptoglobin level after treatment,
Disease status at last follow-up
increasing from undetectable to 20 mg/dL (range, 0-160 mg/dL;
Three responder patients (23%) experienced a recurrence of
mean, 44 Ϯ 55 mg/dL) 2 months after start of treatment.
hemolysis at 7, 8, and 10 months after the first rituximab infusion,
In all responding patients corticosteroids and concomitant
respectively. All these children received a second treatment course
immunosuppressive drugs were progressively tapered and stopped,
with rituximab and all achieved a second disease remission. One of
in 10 of them at a median time of 12 weeks (range, 9-25 weeks).
these children subsequently received a third and a fourth course of
The 10 patients with sustained response are free from any
rituximab, due to further relapses of hemolysis, with a new positive
Immunophenotype analysis
The remaining 10 patients (77% of the responders) are alive and
free from immunosuppressive drugs at a median of 13 months after
Pretreatment absolute number of B lymphocytes was 0.7 ϫ 109/L
treatment (range, 10-28 months). At time of last follow-up, median
(range, 0.25-1.6 ϫ 109/L; normal values in our laboratory being
Hb level in this subgroup of patients was 12.3 g/dL (range, 10-14.7
0.15-0.8 ϫ 109/L), with the median percentage of B lymphocytes
g/dL) and median reticulocyte count was 57 ϫ 109/L (range,
being 22% (range, 14%-39%; normal values in our laboratory
21-73 ϫ 109/L). Also total and direct bilirubin, as well as lactic
being 5%-20%). After treatment, B lymphocytes became undetect-
dehydrogenase and haptoglobin, were within the normal ranges
able in all patients, without any difference between responders and
(data not shown). Nevertheless, DAT remains positive in 3 of these
nonresponders (Figure 2B). As expected, no significant modifica-
10 patients (30%) and IAT is positive in 2 (20%).
tion in the levels of CD3ϩ, CD4ϩ, and CD8ϩ cells were documented.
B-lymphocyte count returned to normal 6 months after treat-
ment in 10 of the 15 patients (67%), whereas it was still below thenormal range in 5 (33%; Figure 2B). Possibly due to the relatively
Discussion
limited number of patients, no statistically significant correlationwas observed between the B-lymphocyte number 6 months after
The anti-CD20 MoAb rituximab has been shown to be effective for
treatment and the risk of recurrence of hemolysis in the 13
the treatment of B-cell malignancies, in particular low-grade
lymphomas.3,6,7,20 More recently, this new agent was described, inpreliminary reports, as a possible promising treatment for patientswith refractory AIHA.9-18,21 However, treatment of a rather limitednumber of patients was reported, with heterogeneous clinicalfeatures and a relatively short follow-up period. Only the study ofQuartier et al9 evaluated the efficacy of rituximab on a relativelyhomogenous group of 6 children with AIHA.
In our trial, the efficacy and safety of rituximab was prospec-
tively evaluated in the largest series of children with AIHA reportedso far. Whereas in the paper by Quartier et al9 all patients achieved
Figure 2. Haptoglobin and absolute B-lymphocyte counts. Pretreatment and
sustained remission, in our cohort rituximab was not effective in 2
2-month posttreatment levels of haptoglobin (A) and pretreatment, 2-month posttreat-
patients and 3 more children had relapses. Remarkably, our study
ment, and 6-month posttreatment absolute B lymphocyte counts (B), as well as mean
population comprised a significant number of very young patients,
values Ϯ SD for the whole study population. Small circles indicate the value for eachpatient; large circles, median values for the entire study population.
the median age at diagnosis being 2 years. In children with onset of
AIHA before the age of 2 years the course of disease is commonly
humoral immunity, was successfully cured with administration
protracted and immunosuppressive treatment is not consistently
effective and carries a risk of death from infections.2,9 In our cohort
Compared with the other immunosuppressive agents used for
of patients, only 1 of the 8 children younger than 2 years of age was
the treatment of antibody-mediated autoimmune disorders, ritux-
refractory to treatment with rituximab. On the other hand, 2 of the 3
imab presents the advantage of inducing selective B-cell immuno-
relapses occurred in this subgroup of patients.
suppression, sparing cellular immunity mediated by T cells and
Rituximab could be safely readministered in the 3 patients with
natural killer (NK) cells. The specific impairment of antibody
relapses, confirming the low immunogenicity of the MoAb due to
production can be easily corrected by prophylactic intravenous
its human component, which would not preclude retreatment.
immunoglobulin administration, which allows maintenance of
As concerns the type of autoantibody responsible for the
normal IgG levels for the whole period of B-cell depletion. For this
hemolysis, Finazzi, reviewing the data available in the literature,
reason, we gave replacement therapy with intravenous immuno-
suggested that a better response could be achieved in patients with
globulins. However, the need for prophylactic infusion of immuno-
cold-agglutinin disease, as compared with warm-autoantibody
globulins has not been proved in a controlled study and most
AIHA.22 In our study population, only one child had cold-
patients treated with rituximab for B-cell malignancies did not
agglutinin disease; this child had a good response to the treatment,
but had a relapse 7 months after the first course of rituximab.
The mechanism by which treatment with rituximab is effective
In the study published by Quartier et al,9 all patients received at
in AIHA is still not completely defined. The simplest explanation is
least 4 infusions of rituximab, which is the standard schedule of
that the source of pathogenetic antibodies is removed. However,
treatment used in patients with B-cell malignancies. However,
some studies on other autoimmune diseases did not show any
because B cells have been reported to disappear from peripheral
correlation between the decline of autoantibody levels and re-
blood as soon as after 2 to 3 doses of rituximab,10 most of our
sponse,26,27 suggesting that additional mechanisms involving anti-
patients were given 3 infusions of the MoAb, thus reducing costs.
gen presentation and help to T cells are involved.
One possible reason for concern regarding this form of treat-
In conclusion, our data indicate that rituximab is effective in
ment is represented by the prolonged impairment of antibody
reducing or even abolishing hemolysis in most pediatric patients
production, leading to an increased risk of viral and bacterial
with AIHA and that a sustained response can be achieved in the
infections. Pure RBC aplasia due to parvovirus B19 infection has
majority of cases. Moreover, the effects of prolonged therapy with
been reported after administration of rituximab,8,23 as well as acute
steroids (growth impairment, fluid retention, avascular necrosis of
viral hepatitis B24 and bacterial pneumonia.25 In our series of
bone) or other nonspecific immunosuppressive drugs (eg, life-
patients, we did not observe an increased risk of infectious
threatening infections) are avoided. Recurrence of the hemolysis
complication. Only one child had primary VZV infection, 2 months
may occur, but a second treatment course is feasible and may be
after rituximab infusion. This infection, despite the impairment of
successful in controlling the disease. References
1. Ware RE, Rose WF. Autoimmune hemolytic ane-
10. Zecca M, De Stefano P, Nobili B, Locatelli F. Anti-
antibody (rituximab) for life-threatening autoim-
mia. In: Nathan DG, Orkin SH, eds. Nathan and
CD20 monoclonal antibody for the treatment of se-
mune haemolytic anaemia in a patient with sys-
Oski’s Hematology of Infancy and Childhood.
vere, immune-mediated, pure red cell aplasia and
temic lupus erythematosus. Br J Haematol. 2002;
Philadelphia, PA: Saunders; 1998:499-522.
hemolytic anemia. Blood. 2001;97:3995-3997.
2. Heisel MA, Ortega JA. Factors influencing prognosis
11. Ahrens N, Kingreen D, Seltsam A, Salama A.
19. Hannet I, Erkeller-Yuksel F, Lydyard P, Deneys V,
in childhood autoimmune hemolytic anemia. Am J
Treatment of refractory autoimmune haemolytic
DeBruyere M. Developmental and maturational
Pediatr Hematol Oncol. 1983;5:147-152.
anaemia with anti-CD (rituximab). Br J Haematol.
changes in human blood lymphocyte subpopula-tions. Immunol Today. 1992;13:215-218.
3. McLaughlin P, Grillo-Lopez AJ, Link BK, Levy R,
Czuczman MS, Williams ME. Rituximab chimeric
12. Bauduer F. Rituximab: a very efficient therapy in
20. Coiffier B, Lepage E, Brie`re J, et al. CHOP che-
anti-CD20 monoclonal antibody therapy for re-
cold agglutinins and refractory autoimmune hae-
motherapy plus rituximab compared with CHOP
lapsed indolent lymphoma: half of patients re-
molytic anaemia associated with CD20-positive,
alone in elderly patients with diffuse large-B-cell
spond to a four dose treatment program. J Clin
lymphoma. N Engl J Med. 2002;346:235-242.
21. Mc Mahon C, Babu L, Hadgson A, Hayat A, Con-
nell NO, Smith OP. Childhood refractory autoim-
4. Reff ME, Carner K, Chambers S, et al. Depletion
13. Zaja F, Iacona I, Masolini P, et al. B-cell depletion
mune haemolytic anaemia: is there a role for anti-
of B-cells in vivo by a chimeric mouse monoclonal
with rituximab as treatment for immune hemolytic
CD20 therapy (rituximab)? Br J Haematol. 2002;
antibody to CD20. Blood. 1994;83:435-445.
anemia and chronic thrombocytopenia. Haemato-
5. Byrd JC, Waselenko JK, Maneatis TJ, et al. Ritux-
22. Finazzi G. Rituximab in autoimmune cytopenias: for
imab therapy in hematologic malignancy patients
14. Ship A, May W, Lucas K. Anti-CD20 monoclonal
which patients? Haematologica. 2002;87:113-116.
with circulating blood tumor cells: association with
antibody therapy for autoimmune hemolytic ane-
23. Sharma VR, Fleming DR, Slone SP. Pure red cell
increased infusion-related side effects and rapid
mia following T cell-depleted, haplo-identical
aplasia due to parvovirus B19 in a patient treated
blood tumor clearance. J Clin Oncol. 1999;17:791-
stem cell transplantation. Bone Marrow Trans-
with rituximab. Blood. 2000;96:1184-1186.
24. Dervite I, Hober D, Morel P. Acute hepatitis B in a
6. Coiffier B, Haioun C, Ketterer N, et al. Rituximab
15. Iannitto E, Ammatuna E, Marino C, Cirrincione S,
patient with antibodies to hepatitis B surface anti-
(anti-CD20 monoclonal antibody) for the treat-
Greco G, Mariani G. Sustained response of refrac-
gen who was receiving rituximab. N Engl J Med.
ment of patients with relapsing or refractory ag-
tory chronic lymphocytic leukemia in progression
gressive lymphoma: a multicenter phase II study.
complicated by acute hemolytic anemia to anti-CD20
monoclonal antibody. Blood. 2002;99:1096-1097.
25. Rosenthal E, Karsenti J-M, Pesce A, Cassuto JL.
Anti-CD20 monoclonal antibody (rituximab) ad-
7. Leget GA, Czuczman MS. Use of rituximab, the
16. Morselli M, Luppi M, Potenza L, et al. Mixed warm
ministration in patients with refractory immuno-
new FDA-approved antibody. Curr Opin Oncol.
and cold autoimmune hemolytic anemia: com-
logic thrombocytopenic purpura [abstract]. Blood.
plete recovery after 2 courses of rituximab treat-
8. Song KW, Mollee P, Patterson B, Brien W, Crump
26. Edwards JCW, Cambridge G. Sustained improve-
M. Pure red cell aplasia due to parvovirus follow-
17. Cohen Y, Polliack A, Zelig O, Goldfarb A. Mono-
ment in rheumatoid arthritis following a protocol
ing treatment with CHOP and rituximab for B-cell
therapy with rituximab induces rapid remission of
designed to deplete B lymphocytes. Rheumatol-
lymphoma. Br J Haematol. 2002;119:125-127.
recurrent cold agglutinin-mediated hemolytic anemia
9. Quartier P, Brethon B, Philippet P, Landman-
in a patient with indolent lympho-plasmocytic lym-
27. Stasi R, Pagano A, Stipa E, Amafori S. Rituximab
Parker J, Le Deist F, Fischer A. Treatment of
phoma. Leuk Lymphoma. 2001;42:1405-1408.
chimeric anti-CD20 monoclonal antibody treat-
childhood autoimmune haemolytic anaemia with
18. Perrotta S, Locatelli F, La Manna A, Cennamo A,
ment for adults with chronic idiopathic thrombocy-
rituximab. Lancet. 2001;358:1511-1513.
De Stefano P, Nobili B. Anti-CD20 monoclonal
topenic purpura. Blood. 2001;98:952-957.
Adopted by NZDA Board March 2003 CODE OF PRACTICE ANTIBIOTIC PROPHYLAXIS FOR DENTAL TREATMENT OF PATIENTS WITH PROSTHETIC JOINT REPLACEMENTS 1. INTRODUCTION Prosthetic replacement of large joints such as the hip, knee, elbow and shoulder is an increasingly common and highly successful orthopaedic surgical procedure. Haematogenous infection of a prosthetic joint replacement is a devas
SURF LIFE SAVING AUSTRALIA POLICY STATEMENT INTRODUCTION Asthma is a common condition in Australia, affecting 12.8% of the population1. It is more common in school aged children than adults2. Currently there is no cure for asthma but in the majority of cases it can be well controlled so that the person with asthma has no limitations in their life. There are many examples of stat
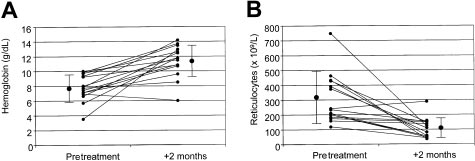 Table 2. Therapies administered before rituximab treatment
Table 2. Therapies administered before rituximab treatment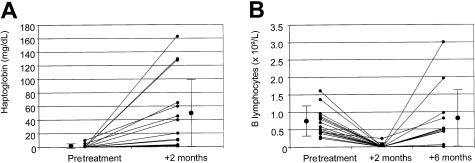 BLOOD, 15 MAY 2003 ⅐ VOLUME 101, NUMBER 10
Table 3. Details of treatment with rituximab and results
BLOOD, 15 MAY 2003 ⅐ VOLUME 101, NUMBER 10
Table 3. Details of treatment with rituximab and results