Double-Blind Placebo Controlled Crossover Study of Clotrimazole
Week for Six Weeks in the Treatment of Rheumatoid Arthritis
Clotrimazole has a broad spectrum of anti-mycotic activity and
was developed clinically for its control of fungal infections,
pathogenic for animals and man. The drug was developed as an agent
by Bayer Laboratories from a screening program involving more than
900 substituted imidazoles active against dermatophytes, yeasts,
Clotrimazole has also been shown to have anti-protozoal action
and it has been suggested that chemical compounds which have anti-
protozoal activity are useful when administered internally for
treating rheumatoid arthritis (1). It has also been suggested that
this may be one of the most effective agents of this class for
treating rheumatoid arthritis (1,2).
Clotrimazole is an antimycotic drug, synthesized by the Bayer
Laboratories in Elberfeld, Germany, by M. Plempel et al (3), known
as Bayb 5097, also known as canesten or lotrimin (Delbay U.S.A.) It
is chemically bis-phenyl (2-chlorphenyl)-1-imidazolyl-methane and
is approved by the U.S. Food and Drug Administration only for
topical treatment of tinea and candida infections of the skin. It Is
available as a 1% solution or cream for external use. Clotrimazole
has an in vitro activity and inhibits growth of most strains of the
various dermatophytes that cause tinea pedis, tinea crurisand tinea
corporis. It also inhibits the growth of some strains of
gram-positive bacteria and has activity against trichomonas species
in high concentrations (4). Clotrimazole is also available in 100 mg.
vaginal tablets and it is reported to be active against vaginal
Oral clotrimazole has been used successfully to treat systemic
mycotic infections in broad series of clinical trials with divided
dosage ranging from 40-100 mg/kg/day (6). Side effects are primarily
gastrointestinal with upper GI discomfort, nausea and diarrhea a
significant limiting factor in 1/3 of patients. CNS effects are seen
in up to 8% of patients consisting of apathy, depression and in rare
Since the anti-helmintic imidazole levamisole has been widely used
in the treatment of rheumatoid arthritis, much has been learned which
can be applied to studies of the effects of other agents of a similar
class in the treatment of patients with this disease (7). Early in the
course of trials with this agent, daily dosage was employed with a
distressing 10% of patients developing severe neutropenia (8). With
the development of regimens utilizing several days per week or one day
per week therapy a lower incidence of hematologic problems has been
demonstrated although this drug continues to have too high an inci-
dence of side-effect development to be widely used in the treatment of
rheumatoid arthritis at present (9,10). Another imidazole, metronida-
zole has been tried in rheumatoid arthritis without significant side
effects but with doubtful efficacy (11). Clotrimazole in high doses
has been shown to be effective in the treatment of rheumatoid arthri-
tis but its use has been associated with an unacceptably high inci-
dence of side effects (2). Since it has been suggested in an uncon-
trolled study that lower doses may be effective in the treatment of
rheumatoid arthritis (1), this trial will be undertaken at lower doses
to test the efficacy of this drug in rheumatoid arthritis.
An in depth discussion of the chemistry, toxicology, and pharma-
cology, of clotrimazole is included in Appendix T. A detailed
bibliography for this protocol is included as Appendix J.
To evaluate the efficacy and tolerability of clotrimazole 20mg/
kg given in q.i.d. divided dosage for two consecutive days per week
for six weeks compared to placebo given in the same schedule in a
double-blind study in the treatment of patients with active rheuma-
Patients with diagnosis of rheumatoid arthritis on stable
dosages of aspirin or non-steroidal anti-inflammatory agents for at
]east one month will he enrolled in this trial. Patients must meet
the criteria for definite or classical rheumatoid arthritis as
Patients must have active disease as indicated in Appendix B
and must agree to attempt to continue on their nonsteroidal anti-
inflammatory drugs at the same dosage during the duration of the
The presence of arthritis due to the ARA exclusions listed in
Patients who do not show active disease as indicated in
Pregnant females or nursing mothers.
Cirrhosis, hepatitis, or liver enzyme abnormalities more
than 20% above the upper limits of normal
Patients who are being treated with or who have been treated
in the last three months with immunomodulating agents (gold, peni-
cillamine, antimalarials, corticosteroids, or cytotoxic agents
Forty patients will be entered in this double-blind crossover
Duration of clinical trial is 1 year.
Duration of study for each patient is six months as follows:
six weeks on medication or placebo followed by six weeks observa-
tion, followed by six weeks on medication or placebo, followed by
History and physical.Complete history and physical examina-
tion will be obtained at visits one and nineteen.
Patients will he numbered consecutively as they are entered
into the study. By random allocation, one-half of the patients will
receive clotrimazole in 250 mg. compressed tablets in the dose of 20
mg/kg in four divided doses, taken two consecutive days per week for
the period of six weeks. One-half of the patients will receive
identical placebo tablets. This will he followed by a six week wash-
out/observation period. At the end of 12 weeks, patients will be
crossed over and receive the alternative placebo or trial medica-
tion. This will also he followed by a six week observation period.
The randomization process will be performed at visit one.
At visit one, a bottle containing either active medication
placebo tablets will he dispensed to each patient. Directions on
the bottle will read, “Take as directed.” The patients will he given
written instructions to take six to eight tablets per day, depend-
ing on their body weight as equally divided q.i.d. doses. Medica-
tions will be dispensed at each visit, and the number of
tablets will be recorded on the Clinical and Laboratory Assessment ofDisease Activity Sheet: (Appendix C) for each visit. No changes in
anti-inflammatory agent medication will he allowed during the study.
Injectable corticosteroids are not allowed during the study. Pure
analgesics such as acetaminophen will he allowed during the study
but notation of the number of tablets taken will be noted on the
clinical and laboratory assessment sheet.
The same study technician will evaluate a given patient with the
help of one of the rheumatology physicians and compile the data in
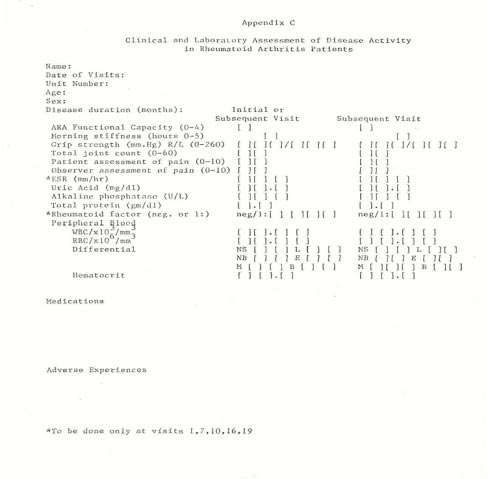
Appendix C at the same time of day at each visit. Demographic data
will be entered as indicated giving the patient’s name, visit date,
unit number, age, sex, and duration of disease. The anti-inflamma-
tory agent medication, analgesic medication, number of study cap-
sules returned and number consumed will be recorded if appropriate,
on the Assessment Sheet (Appendix C). The American Rheumatism Asso-
ciation functional class 0 to 4 will be determined as indicated in
Appendix D and recorded on the Assessment Sheet. Morning stiffness
will be entered in units of one hour from zero to five. Grip
strength readings from each hand will be recorded separately in mm/
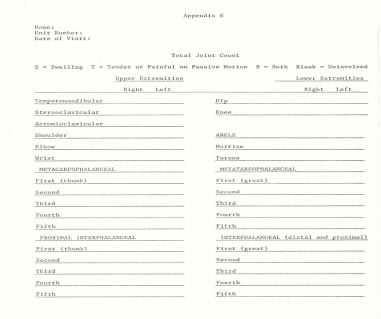
Hg from 0 to 260. A Total Joint Count Recording Sheet (see Appendix
E) will be used to evaluate the total number of joints involved and
the value (0 to 60) will he entered on the Assessment Sheet. A joint
will be considered affected if objective findings such as tender-
ness, pain on passive motion, or swelling are noted on examination.
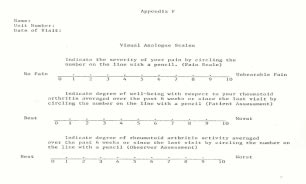
Pain intensity, patient assessment, and observer assessment will be
quantitated using visual analogue scales. Patients will indicate
the severity of their pain at each visit on an 11 point scale (see
Appendix F). Patient and observer assessment will be evaluated
using similar measurements (see Appendix F). Laboratory data in-
cluding Westergren ESR, uric acid, alkaline phosphatase, total
protein, and rheumatoid factor titer will be recorded on the As-
sessment Sheet. Peripheral blood WBC/mm3, differential leukocyte
count, and hematocrit readings will also be entered on the Assess-
ment Sheet. Clinical efficacy and side effect evaluations will be
performed at each visit and will be recorded on the Assessment Sheet
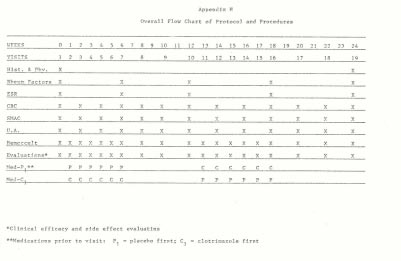
The following laboratory analyses will be performed for safety
Blood and urine specimens will be obtained at the initial
visits and every two weeks for the following:
SMAC - See Appendix C for methods and normal ranges Routine
Hemoccult cards will be given to the patient to test for
occult blood, and these cards will be checked at each visit. Results
from at least one specimen should be recorded each week. Other
results can be recorded if more are obtained.
Westergren sedimentation rates and rheumatoid factors will be
done at visit one, seven, ten, sixteen, and E.
Adverse experiences are defined as any unwanted signs or symptoms
which may in any way be related to pharmacologic action of any of
the drugs taken by the patient. All such experiences are to be
entered on the Clinical and Laboratory Assessment Sheet (Appendix
C) with the following data to he recorded: onset date, duration,
frequency, drug relationship, and action taken. Any adverse experi-
ences should be reported immediately to Dr. Robert Turner or the
Rheumatology Fellow on call at (919) 748-4209.
An effort will be made to determine the reason for each dropout
and complete history and physical examination will be performed at
the beginning of the study and at the study termination, listing the
investigators’ opinion as to how the patient did on the study, any
adverse experiences encountered, and the patient and observer opin-
ion as to the efficacy of the medication utilized at each time
An overall flow chart of the protocol and procedures for this
Data analysis will be performed as follows:
Forty subjects (S .S ) will be randomly divided into 2 groups
of 20 (Groups 1 and 11.) consisting of subjects S* .S*
respectively (Statistical Tables Appendix K). Group I and Group
II). Group I and II subjects will receive drug, placebo or neither
according to the scheme outlined in Appendix H. Data collected per
Appendix C will be recorded in parallel for each Group at visits 1,
7 , 1 0 , 1 6 , a n d 1 9 . S t a t i s t i c a l c o m p u t a t i o n s w i l l b e
performed on an IBM PC-XT computer using LOTUS 1,2,3, electronic
spreadsheets for data recording and manipulations. Each measured
parameter at visits 7, 10, 16 and 19 will be compared with its value
at visit 1 using the paired t-test (19). This test will reveal
significant effects of drug or placebo on rheumatoid arthritis
activity disease parameters within each group. Each parameter will
also be tested for stability by analysis of variance using the
treatment-by-subjects design (20) in which the parameter is evalu-
ated over the course of the protocol by computation of an F
statistic. The F value will be computed for data collected on
visits 1, 7, 10, 16 and 19. A significant F value indicates that the
parameter was not stable during the protocol. These two tests of
significance should allow a preliminary evaluation of the effects
of drug on the disease activity parameters. Negative results would
strongly suggest lack of effect. Positive results in one or more
tests would indicate that further data analysis (e.g., intergroup
comparisons) is warranted. In this circumstance outside statistical
A. Criteria for the classical of rheumatoid arthritis
This diagnosis requires 7 of the following criteria. In criteria
1 through 5 the joint signs or symptoms must he continuous for at
least 6 weeks. Any one of the features listed under Exclusions (See
below) will exclude a patient from this and ail other categories.
Pain on motion or tenderness in at least 1 joint (observed by
Swelling (soft tissue thickening or fluid, not bony over-
growth alone) in at least 1 joint (observed by a physician).
Swelling (observed by a physician of at least 1 other joint
(any interval free of joint symptoms between the 2 joint involve-
ments may not be more than 3 months).
Symmetric joint swelling (observed by a physician) with si-
multaneous involvement of the same joint on both sides of the body
(bilateral involvement of proximal interphalangeal, metacarpopha-
langeal, or metatarsophalangeal joints is acceptable without abso-
lute symmetry). Terminal phalangeal joint involvement will not
prominences, on extensor surfaces, or in juxtaarticular regions.
Roentgenographic changes typical of rheumatoid arthritis (which
must include at least bony decalcification localized to or most
marked adjacent to the involved joints and not just degenerative
changes). Degenerative changes do not exclude patients from any
group classified as having rheumatoid arthritis.
Positive agglutination test. Demonstration of “rheumatoid fac-
tor” by any method which, in 2 laboratories, has been positive in
not over 5% of normal controls, or positive streptococcal aggluti-
Poor mucin precipitate from synovial fluid (with shreds and
solution). An inflammatory synovial. effusion with 2,000 or more
white cells/mm3, without crystals can be substituted for this cri-
Characteristic histologic changes in synovium with 3 or more
of the following: marked villous hypertrophy; proliferation of
superficial synovial cells often with palisading; marked infiltra-
tion of chronic inflammatory cells (lymphocytes or plasma cells
predominating) with tendency to form “lymphoid nodules”; deposition
of compact fibrin either on surface or interstitially; foci of
Characteristic histologic changes in nodules showing granu-
lomatous foci with central zones of cell necrosis, surrounded by a
palisade of proliferated mononuclear and peripheral fibrosis and
chronic inflammatory cell infiltration.
This diagnosis requires 5 of the above criteria. In criteria 1
through 5 the joint signs or symptoms must be continuous for at
The typical rash of systemic lupus erythematosus (with but-
terfly distribution, follicle plugging, and areas of atrophy).
High concentration of lupus erythematosus cells (4 or more in
2 smears prepared from heparinized blood incubated not over 2
Histologic evidence of periarteritis nodosa with segmental
of arteries associated with nodular leukocytic infiltration
extending perivascularly and tending to include many eosinophils.
Weakness of neck, trunk and pharyngeal muscles or persistent
Definite scleroderma (not limited to the fingers).
A clinical picture characteristic of rheumatic fever with
migratory joint involvement and evidence of endocarditis, espe-
cially if accompanied by subcutaneous nodules or erythema marginatum
or chorea. (An elevated antistreptolysin titer will not rule out
the diagnosis of rheumatoid arthritis).
A clinical picture characteristic of gouty arthritis with
acute attacks of swelling, redness, and pain in 1 or more joints,
especially if relieved by colchicine or accompanied by urate crys-
A clinical picture characteristic of acute infectious ar-
thritis of bacterial or viral origin with: an acute focus of infec-
tion or in close association with a disease of known infectious
origin, chills, fever, and an acute joint involvement, usually
migratory initially (especially if there are organisms in the joint
fluid or response to antibiotic therapy).
Tubercule bacilli in the joints or histologic evidence of
A clinical picture characteristic of Reiter’s syndrome with
urethritis and conjunctivitis associated with joint involvement,
A clinical picture characteristic of the shoulder-hand syn-
drome with unilateral involvement of shoulder and hand, with dif-
fuse swelling of the hand followed by atrophy and contractures.
A clinical picture characteristic of hypertrophic osteoar-
thropathy with clubbing of fingers and/or hypertrophic periostitis
along the shafts of the long bones especially if an intrapulmonary
lesion (or other appropriate underlying disorder) is present.
A clinical picture characteristic of neuroarthropathy with
condensation and destruction of bones of involved joints and with
Histologic evidence of sarcoid or positive Kveim test.
Multiple myeloma as evidence by marked increase in plasma
cells in the bone marrow, or Bence-Jones protein in the urine.
Characteristic skin lesions of erythema nodosum.
Leukemia or lymphoma with characteristic cells of periph-
eral blood, bone marrow, or tissues.
Active RA patients must show at least 3 of the following crite-
Number of tender or painful joints on motion =>6
Complete functional capacity with ability to carry on
Class II: Functional capacity adequate to conduct normal activi-
ties despite handicap or discomfort or limited mobility of 1 or more
Functional capacity adequate, to perform only few or
none of the duties of usual occupation or of self care
Class IV: Largely or wholly incapacitated with patient bedridden
or confined to wheelchair, permitting little or no self care
Detailed Discussion of Chemistry, Toxicology, and Pharmacology
This drug is a synthetic tritylimidazole.
1-(2-chloropheny1benzhydry1) imidazole; also bis-
phenyl-(2 chloropheny1-1-imidazoly1 methane.
Weakly alkaline, colorless, crystalline substance which forms stable
salts with both inorganic and organic acids. It is slightly hygro-
In mice and rats death is seen in 24 hours. In rats death occurs
in 2-6 days of weakness, apathy and muscle spasm.
Dogs and cats vomit the drug and no oral LD50 can be established
In rodents 200 mg/Kg/day is tolerated by lavage with minimal
weight loss. At autopsy liver and adrenal hypertrophy is seen with
associated marked increase in microsomal enzyme induction.
Dogs at 100 or 200 mg/Kg/day show emesis and liver and adrenal
SGOT enzyme elevation is seen but no jaundice.
Monkeys receiving 150 mg/Kg/day for 6 weeks develop vomiting,
Rats on chronic study of 50 and 150 mg/Kg/day show SGPT, Alk Phos
elevation, liver enlargement, fatty liver, and adrenal enlargement.
In monkeys and dogs at 12 months post drug liver size returns to
normal but the adrenals remain enlarged for a much longer period
Thirteen healthy volunteers each received 500 mg. Clotrimazole
for 28 days. The preparation was taken orally in capsules soluble in
gastric juice. Before the test and on the 3rd, 7th, 14th, 21st and
28th day hepatic function, protein and fat metabolism, renal func-
tion and the peripheral blood-picture were examined. At the same
time the volunteers were questioned about the subjective tolerance.
Due to gastro-intestinal intolerance, the starting dose of 60 mg/
Kg/day could not he maintained. Subjective side effects were less
on a lower dose. In one case there was a rise in liver transaminases
and in one there were leukopenia. Both stopped treatment.
There were six males (mean 25 years) and seven females (mean 37
years). The drug was given three times daily after meals. Nine of
the volunteers completed the 28 day trial. Of the other four, one
stopped on the 3rd day, one on the 4th day and two on the 21st day
of the trial. Three groups of side effects were observed.
including nausea, vomiting, anorexia a n d
Central nervous, including lethargy, depression and irrita-
Of the two subjects who discontinued the trial due to changes in
biochemical parameters, one showed an increase in SGOT to 36.5
I.U., and in SGPT to 58.2 I.U. on the 21st day of treatment. Seven
days later the SGOT had returned to normal and the SGPT was still
slightly raised. In the second, the base line leukocyte count was
3,600 which fell to 2,400 on the 21st day. At the same time the
alkaline phosphatase fell sharply. Seven days later the blood pic-
ture had returned to normal and the alkaline phosphatase was 1 mU/
For those completing the trial there was a change in nearly all
parameters, with the exception of α -, α - and γ-globulins, and SGPT
3rd day: Fall in erythrocytes, haemoglobin, leukocytes (with
relative lymphocytosis) total cholesterol and total protein; in-
crease in phosphatides, urea, bilirubin, and free glycerine.
Esterified fatty acids, lipoproteins, alkaline phosphatase and
SGOT increased; free glycerine, total cholesterol plasma proteins
Blood picture relapsed, SGOT and bilirubin raised.
F a t m e t a b o l i s m n o t i n v e s t i g a t e d . T o t a l p r o t e i n
decreased; but relative increase in “pre-albumin.”
Haemoglobin raised, bilirubin normal. Erythrocyte down,
white blood count normal. Phosphatides and enzymes normal. In-
creases in lipid fractions and urea; total protein still low; low“pre-albumin” fraction, raised globulin fraction.
The increase in blood urea is within the norm and is probably
without clinical significance, since kidney function remains nor-
mal. It is suggested, however, that in patients with impaired renal
function, blood urea and creatinine should be checked regularly.
From the measurements of ketosteroid excretion, there is no evi-
dence of interference with adrenal function after administration of
In a second study 7 healthy women received 3.0 G clotrimazole
orally/day for 14 days. Two developed anorexia, one with nausea and
vomiting. Apart from a rise in the alkaline phosphatase of one
patient to 32.6, monitoring was normal.
On the isolated guinea pig intestine concentrations above 3 x 10-
7 cause inhibition of the contractions evoked by ricotine, acetyl-choline, histamine and barium chloride. An intramuscular dose of 10
mg/Kg has no effect on gastric secretion in the rat, nor has an oral
dose of 100 mg/Kg any purgative effective. 50 mg/Kg given
intraduodenally has no choleretic action. An oral dose of 100 mg/Kg
An oral dose of 1000 mg/Kg in the mouse has no mydriatic action,
no anti-convulsive action, and no inhibition of a defense reaction.
It has a mild sedative effect. An oral dose of 400 mg/Kg in the
rabbit has no hypnotic action as gauged by the EEG response.
Clotrimazole given to cats at 100 and 200 mg/Kg produced pronounced
central excitation, similar to that of anti-depressants.
Prolonged administration did not alter the blood sugar in rats or
dogs. However, in acute experiments high doses lowered the blood
sugar. The blood sugar of mice given five doses of 250 mg/Kg falls
at 3 hours to 116 mg% compared to a control value of 150 mg%.
In fed but not starved rats there is a significant reduction in
blood sugar at 2 and 4 hours after single doses up to 250 mg/Kg, the
reduction increasing with increased number of doses and lasting up
Adrenalectomised rats show a greater fall in blood sugar on
corresponding doses. Tolbutamide causes a similar fall (40%) in
blood sugar in rats rendered hypoglycemic on clotrimazole to the
fall produced in untreated rats. Clotrimazole induced hypoglycemia
is not brought about by a release of insulin, as there is no
concomitant fall in non-esterified fatty acids.
Absorption, Distribution and Excretion in Animals
C-14 labelled clotrimazole was given orally to 46 rats. Absorp-
tion of a 30 mg/Kg dose was greater than 90%. One hour after
administration radioactivity was concentrated in the skin, liver,
adrenal cortex, adipose tissue, gastric mucosa and proximal small
intestine. The metabolites are excreted in the bile and 90% is
eliminated via the faeces. After a single dose there is only 1%
activity in the body after four days. There is no secretion of
intact clotrimazole either in the bile or the urine.
The main metabolites are bisphenyl-2-chlorophenylmethane, 2
c h l o r o p h e n y l - 4 1- h y d r o x y p h e n y l - p h e n y l - m e t h a n e , b i s p h e n y l - 2 -
chlorophenyl methanol, and 2 chlorobenzophenone.
C-14 labelled clotrimazole given orally to 2 dogs resulted in
very low peak concentrations in the blood. The excretion of activ-
ity was predominantly via the faeces.
The excretion of clotrimazole metabolites in mice reached peak
values from 10-16 hours after administration. The urinary excretion
of metabolites was 5% of the dose administered.
Exception tests were carried out with cats, dwarf hogs and cattle.
The results were comparable. None of the animal species tested was
found to secrete unaltered clotrimazole in the urine, as shown by
microbiological assay. On intra-peritoneal and subcutaneous adminis-
tration, little of the preparation is absorbed. The resulting urinary
excretions are less than 1 µg metabolite/ml urine.
Serum concentrations were determined after single and repeated
administration of clotrimazole in mice, rats, guinea pigs, dwarf
hogs, dogs and cattle. Peak serum concentrations obtained in mice and
rats after single oral dose of 100 mg/Kg are obtained 3-5 hours after
On the third day of receiving 100 mg/Kg/day, the blood levels of two
dwarf hogs were between 6 and 8 µg per ml four hours after the lastdose. Serum levels for beagle dogs two hours after the last dose in
the 100 mg/Kg group ranged from 3-6 µg/ml, and in the 50 mg/Kg group,from 2-3 µg/ml.
After beagle dogs had received 100 mg/Kg for 13 weeks, clotrimazole
(or metabolite) concentrations were determined in tissue extracts
by chromatography. The concentration was 2-3 µg/G of fresh tissuefor heart, lung and kidney. Liver contained 7 µg/G, approximatelytwo-thirds of which were metabolites. Bile contained 12 µg/ml asmetabolites only. Adipose tissue contained 20 µg/G clotrimazoleand/or its metabolites.
Five groups of 50 male and 50 female rats were treated with
Clotrimazole 0, 10, 25, 60 and 150 mg/Kg/day and examined at 6
months. Up to 6 months no adverse effect was apparent except a
At 6 months females showed some reduction in haematocrit and
haemoglobin and a rise in cholesterol. Males in one group had
lowered cholesterol levels. Liver weights were increased in both
sexes, the livers being fatty. Microscopy showed hepatocellular
swelling, increased granularity of the cytoplasm and hyperchromatic
nuclei. There were no mitotic figures nor bile stasis. Other organs
None seen at chronically tolerated dosage in mice, rats or rab-
Groups of 10 male and 20 female rats were fed the following doses
of clotrimazole: 0, 5, 10, 25, and 50 mg/Kg/day throughout. After
ten weeks two females were put with one male for a week in rotation
so that each female was exposed to 3 different males for one oestrus
cycle. After successful impregnation or 3 weeks the animals were
separated. Some rats were delivered by Caesarean at 13 days, others
reared their litter to four weeks. Clotrimazole did not impair the
parents’ behavior, health or fertility. Pregnancy was unaltered.
Of 50 rats treated for 348 days (448 life days) with a total dose
of 3.45 g/Kg, four died, each with hepatic degeneration. None
showed any evidence of tumor formation.
There were no significant differences in blood sugar, urea, BSP
retention, SGOT, SGPT, ornithine carbaminoyl-transaminase, cal-
cium, total bilirubin, or heparin recalcification time between
treated and control dogs, or between treated groups of dogs (4 dogs/
group) given 50, 100 or 200 mg/kg for 13 weeks.
The serum alkaline phosphatase rose in a dose dependent manner.
Serum cholesterol was significantly reduced in dogs on 200 mg/Kg
and leucine aminopeptidase was significantly elevated.
Alkaline phosphatase values rose during the 13 weeks clotrimazole
Urine analysis was normal except for continuous proteinuria in
one female on 200 mg/Kg and transient proteinuria in two males on
the same dose and one male each on 100 and 50 mg/Kg.
Final bodyweights and heart sizes were not significantly differ-
ent at necropsy. There was a dose dependent significant increase in
liver and adrenal weights. Kidney weight was only significantly
Histopathology was performed at Huntingdon Research Center with
Liver:Hepatocyte enlargement occurred in all animals including
controls, being more marked in three of the 200 mg/Kg animals.
Degenerative changes seen in rat liver were not seen in the dog
Adrenals: In dogs on 200 and 100 mg/Kg there was cellular en-
largement, particularly in the zona fasiculata.
All other tissues were examined and found to be normal.
A further study with rats was undertaken to assess recovery from
Three groups of 30 male rats were treated five times per week for
six weeks with a single dose of a suspension of 0, 10 and 100 mg/Kg
clotrimazole orally. Three rats from each group were killed after
1,2,5,10,20 and 30 daily doses, then 1, 2, 4, and 10 weeks after the
In the 100 mg/Kg group, epithelial hypertrophy of the liver
developed initially, followed by hyperplasia and low-grade paren-
chymal damage towards the end of treatment. Ten weeks after the
termination of treatment these liver changes were not observed.
Fatty infiltration of the liver was seen in both test and control
groups, being more pronounced in the animals treated with 100 mg/
Kg, and increasing throughout the study.
Repeated oral doses of Clotrimazole given to mice produce an
induction of liver enzymes with a consequent lowering of serum
levels of clotrimazole due to a more rapid catabolism.
Direct evidence comes from the sleeping time of mice given hex-
obarbital. Four groups of 20 mice received i.v. 150 mg/hexobar-
bital/Kg, and the sleeping time measured. Then each received 100
mg. clotrimazole/Kg orally for five days and on the sixth day a
further dose of hexobarbitone, and the sleeping time measured again.
Clotrimazole also induces the parathion-splitting enzyme sys-
tem, which is blocked by DL-ethionine. This block is not reversed by
methionine. Clotrimazole induces enzyme systems in adrenalecto-
mized animals, suggesting that the adrenals are not implicated.
In subacute toxicity tests there was a dose dependent increase in
liver weight and urinary excretion of ascorbic acid, suggesting
that there was an adaptive rather than toxic mechanism responsible;
although the failure of methionine to reverse the effect of DL-
ethionine suggests that the ascorbic acid excretion test does not
differentiate between hyperfunctional and toxic hepatomegaly.
In man, enzyme induction occurs later, within three weeks of
C-14 Clotrimazole was given orally in gelatin capsules to hospi-
talized patients and healthy volunteers. It was well absorbed (90%)
from the gastrointestinaltract. The blood levels achieved were dose-
dependent, reaching a peak around 3 hours. Serum levels over 1 µg/mlof active substance were reached between the third and sixth hour
after dosage. The ratio of active to inactive substance was 1:1.5.
In humans, the active substance was also found in saliva, sputum,
sweat, and subcutaneous fat. The active substance has only been
demonstrated in the cerebrospinal fluid in cases of meningitis.
No active substance, and only 10% metabolites are excreted in the
urine. In infants active substance can be demonstrated in urine
after high doses. Clotrimazole is almost completely metabolized in
the human. The metabolites are excreted predominantly in the bile.
Similar metabolic and distribution results have been reported by
Duhm et al. (13). In clinical studies these workers have used
dosages as high as 3 gms in patients receiving increasing dosages of
25 mg/Kg/day for 12 days with peak serum levels seen in 3 hours.
Vaginal application results in serum levels 500x lower.
Leukocyte myeloperoxidase levels rose in 15 of 17 patients in
another study (14). Effects were seen on the 3rd day in those
receiving clotrimazole. This drug has also been studied in such
widely varying settings as a trial of therapy for oral candidiasis
bronchopulmonary aspergillosis in adults (16), treatment of ocu-
lar aspergillosis (17), and treatment of fungal infection in renal
Wyburn-Mason R. Clotrimazole in Rheumatoid Arthritis.Lancet
Wojtulewski JA, Gow PJ, Walter J, Grahme R, Gibson T, Panayi
GS, Mason J. Clotrimazole in Rheumatoid Arthritis. Ann Rheum Dis
Plempel M, Bartman K, Buchel KH, Rezel E. Experimental Study
of a New Orally Effective Broad-Spectrum Antimycotic Agent. Deutsche
Medizinische Wochenschrlft 94:1356, 1969.
Sawyer PR, Brogden RN, Pinder RM, Splight TM, Avery GS.
Clotrimazole: A Review of its Antifungal Activity and Therapeutic
Schnell .JD. The Incidence of Vaginal Candida and Trichomonas
Infections and Treatment of Trichomonas Vaginitis with Clotrimazole.
Postgrad Med J July Suppl 79-81, 1974.
Hoffbrand BJ, Allan HB, Good CS Editors. Clotrimazole.P r o c
of Conf Royal Coll of Physicians. Postgrad Med J July Suppl 24-108,
Runge LA, Rynes RI. Balancing Effectiveness and Toxicity of
Levamisole in the Treatment of Rheumatoid Arthritis. Clin Exp Rheum
Williams GT, Johnson SAN, Dieppe PA, Huskisson EC. Neutrope-
nia During Treatment of Rheumatoid Arthritis with Levamisole. Ann
Runge LA, Pinals RS, Lourie SH, Tomar RH.Treatment of Rheu-
matoid Arthritis with Levamisole. Arthritis Rheum 20:1445-1448,
Harkness JAL, Griffin AJ, Heinrich I, Gibson T, Grahame R. A
Double-Blind Comparative Study of Metronidazole and Placebo in
Rheumatoid Arthritis. Rheumatol Rehab 21:231-234, 1982.
Tettenbron D. Toxicity of Clotrimazole.Postgrad Med J July
Duhm B, Medenwald H, Peutter J, Maul W, Patzchke K, Wegner
LA. The Pharmacokinetics of Clotrimazole C. Postgrad Med J July
Renz M, Farqutar JW, Cohen M, Harness RA. Elevation of
Mycloperoxidase Activity in Infants with Oral Candidiasis Treated
with Clotrimazole. Postgrad Med J July Suppl: 30-34, 1974.
Cohen M, Harkness RA, Renz M, Farquhar JW. Trials of the Use
of Clotrimazole In the Treatment of Oral Candidiasis In Newborn
Babies. Postgrad Med J July Suppl: 28-30, 1974.
Milne CJR. Mycological Studies in the Use of Clotrimazole in
Bronchopulmonary Aspergillosis and Neonatal and Vaginal Candidi-
asis. Postgrad Med J July Suppl: 20-23, 1974.
Jones BR, Richards AB. Clotrimazole in the Treatment of
Ocular Infection by Aspergillus Fumigatus. Postgrad Med J July
Bewick M, Raper DA. The Diagnosis of Systemic Fungal Infec-
tion in Renal Transplant Patients and Treatment of Clotrimazole.
Postgrad Med J July Suppl: 34-38, 1974.
Snedecor GW and Cochran WB. Statistical Methods, 6th Ed.,
Iowa State University Press, Ames IA, 94-96, 1967.
Bruning JL and Kinta BL. Computational Handbook of Statis-
tics, 2nd Ed., Scott, Foresman and Co., Glenview, IL, 44-48, 1977.
PROSTATE HEIDELBERG - CANCER SUPPORT GROUP Affiliated with the Prostate Cancer Foundation of Australia Newsletter No: 113 Last Meeting: 12th September 2012 COMMITTEE: Prostate Heidelberg supports men with prostate cancer, and their families and carers. The support takes the form of shared experiences and knowledge from books, subscriptions, internet sites and h
Additive Beneficial Effects of Losartan Combined With Simvastatin in the Treatment of Hypercholesterolemic, Hypertensive Patients Kwang Kon Koh, MD; Michael J. Quon, MD, PhD; Seung Hwan Han, MD; Wook-Jin Chung, MD;Jeong Yeal Ahn, MD; Yiel-Hea Seo, MD; Moon Ho Kang, MD; Tae Hoon Ahn, MD; Background —Biological mechanisms underlying statin and angiotensin II type 1 receptor blocker
 Number of tender or painful joints on motion =>6
Number of tender or painful joints on motion =>6
 Complete functional capacity with ability to carry on
Class II: Functional capacity adequate to conduct normal activi-
ties despite handicap or discomfort or limited mobility of 1 or more
Functional capacity adequate, to perform only few or
none of the duties of usual occupation or of self care
Class IV: Largely or wholly incapacitated with patient bedridden
or confined to wheelchair, permitting little or no self care
Complete functional capacity with ability to carry on
Class II: Functional capacity adequate to conduct normal activi-
ties despite handicap or discomfort or limited mobility of 1 or more
Functional capacity adequate, to perform only few or
none of the duties of usual occupation or of self care
Class IV: Largely or wholly incapacitated with patient bedridden
or confined to wheelchair, permitting little or no self care

 Detailed Discussion of Chemistry, Toxicology, and Pharmacology
This drug is a synthetic tritylimidazole.
Detailed Discussion of Chemistry, Toxicology, and Pharmacology
This drug is a synthetic tritylimidazole.