ARTICLE IN PRESS
Journal of Science and Medicine in Sport (2007) xxx, xxx—xxx Arterial oxygen saturation during ascending to altitude under various conditions: Lessons from the field Martin Burtscher Department of Sport Science, Medical Section,University of Innsbruck, Austria
Received 10 January 2007 ; received in revised form 21 June 2007; accepted 5 August 2007
KEYWORDS
When hypoxia increases during ascending in the mountains, ventilatory
control and the related oxygenation may be challenged. The pre-treatment by inter-
mittent hypoxia will elevate ventilation and offset hypoxemia and acetazolamide
may inhibit peripheral chemosensitivity and act through central mechanisms. Tostudy these effects in the field, one well-trained male mountaineer performed four
ascents from low (1300 m) to higher altitude (2600 m): (1) under control conditions,
(2) after intermittent hypoxia, (3) after pre-treatment with acetazolamide, and (4)
after intermittent hypoxia + acetazolamide. When ascending under control condi-
tions a cascading decrease of arterial oxygen saturation (SaO2) has been observed
probably because of the alternating dominance of peripheral and central mech-anisms of ventilatory control. While the pre-treatment with intermittent hypoxiaprolonged the constant SaO2 periods, the intake of acetazolamide eliminatedthis respiratory periodicity. Oxygen desaturation was best prevented by acetazo-lamide which was also associated with faster ascent times compared to controlconditions. 2007 Sports Medicine Australia. Published by Elsevier Ltd. All rights reserved. Introduction
exercise entilatory control, how-ever, is particularly complex during exercise in
Typically, mountaineers ascend from low to higher
hypoxia where the controller depends on the
altitudes. In contrast to exercise at low alti-
interaction among several different mechanisms.
tude they are exposed to continuously increasing
Ventilatory control and the related SaO2 values
hypoxia. Sufficient ventilation is important to main-
might be modified, e.g. by pre-exposure to inter-
tain arterial oxygen saturation (SaO2) and aerobic
mittent hypoxia or the intake of acetazolamide.Short-term intermittent hypoxia has been reportedto increase ventilation and SaO2 during subse-
quent exposure to hypoxia at rest and during
1440-2440/$ — see front matter 2007 Sports Medicine Australia. Published by Elsevier Ltd. All rights reserved.
Please cite this article in press as: Burtscher M, Arterial oxygen saturation during ascending to altitude under variousconditions: Lessons from the field, J Sci Med Sport (2007), doi:
ARTICLE IN PRESS
submaximal exercise in hypoxia probably caused by
(PetCO2; Tidal Wave Sp, Novametrix, Austria) was
enhanced hypoxic chemosensitivity of the periph-
eral chemoreceptors.In contrast, the intakeof acetazolamide provokes metabolic acidosis andincreases the ventilatory response to the exercise
mainly via central chemoreceptors and improvespulmonary gas Although often used
by mountaineers, it is unknown how such inter-
ascents are schematically shown in Origi-
ventions would impinge on the SaO2 course during
ascending to altitude. Thus, the main objec-
tive of this pilot study was the monitoring of
2 values vary rhythmically. The cycle length
after intermittent hypoxia seems to be pro-
prolonged ascent to altitude: (1) under con-
longed and after acetazolamide and intermittent
trol conditions, (2) after intermittent hypoxia,
hypoxia + acetazolamide cycles seems even to dis-
(3) after the intake of acetazolamide, and (4)
appear. In general, each cycle consists of a
after combined intermittent hypoxia and acetazo-
ing altitude, followed by a rather horizontalSaO2 period despite increasing altitude. Afterintermittent hypoxia the constant SaO
is prolonged and starts at a lower threshold. After acetazolamide, the initial SaO
One healthy, well-trained and regularly exercis-
is followed by a slowed continuous decrease of
ing male mountaineer (52 years, 68 kg, 176 cm,
2. After intermittent hypoxia + acetazolamide,
2max ∼ 65 ml/(min kg)) performed four ascents
this slowed decrease starts at somewhat a
from low to higher altitude. He had a nor-
ascent under control conditions from 98% (700 m,
monly susceptible to acute mountain sickness.
rest) to 83% (2600 m, exercise); delta SaO
He normally lived at low altitude (700 m) and
was transported by car to an altitude of 1300 m
12%, after acetazolamide 9%, and after inter-
and from there he ascended to about 2600 m.
mittent hypoxia + acetazolamide also 9%. The
Ascents were performed in the winter season on
average values of heart rates during the four
skis carrying a light backpack (3 kg) with time
ascents were very similar (136 ± 2 b/min). The
intervals of 3 weeks between each ascent. The
time needed for the ascent under control condi-
routes and the track conditions of the four ascents
tions was 132 min (590 m in altitude per hour),
were very similar (solid tracks, temperature: +4
after intermittent hypoxia this time was 128 min
to −4 ◦C, no wind). One month before and during
(609 m/h), after acetazolamide 122 min (639 m/h),
the test period no altitude sojourn above 1800 mwas allowed. The first ascent represents controlconditions. The second was carried out after inter-mittent hypoxic exposures consisting of five timesof 1 h normobaric hypoxia (14% FiO2, equivalentto about 3700 m) on five consecutive days withthe intent to enhance the sensitivity of peripheralchemoreceptors.third was performed aftertwo times 125 mg intake of acetazolamide within atime interval of 9 h with the intent to enhance thesensitivity mainly of the central chemoreceptoreffectiveness of such low dosages havebeen demonstrated and is also indicated becausediuresis increased. The fourth ascent was per-formed after intermittent hypoxia + acetazolamidepre-treatment. Figure 1 Schematically presented SaO2 courses during
SaO2, barometric pressure, and heart rates were
the ascents from about 1300 m (arrow) to about 2600 m
monitored continuously using the Physiolog device
under various conditions. IH = intermittent hypoxia;
(Driesen + Kern GmbH, Germany). End-tidal CO2
Please cite this article in press as: Burtscher M, Arterial oxygen saturation during ascending to altitude under variousconditions: Lessons from the field, J Sci Med Sport (2007),
ARTICLE IN PRESS
Arterial oxygen saturation under various conditions
and after intermittent hypoxia + acetazolamide
In conclusion, intermittent hypoxia and aceta-
zolamide modify the cascading decrease of SaO2when ascending to altitude under control condi-tions probably because of their selective effects
Discussion
on peripheral and central mechanisms of ventila-tory control. These interventions tend to improve
The most interesting observations of the presented
pilot study are (1) that the SaO2 course duringascending to altitude follows a biphasic patternand (2) that intermittent hypoxia, acetazolamide,
Appendix A. Supplementary data
and intermittent hypoxia + acetazolamide clearlychanged the rhythmic variation of the SaO2 course
Supplementary data associated with this arti-
seen during the control ascent to altitude.
cle can be found, in the online version, at
(1) Under control conditions, constant SaO2 peri-
ods with rather decreasing PetCO2 may reflectincreasing ventilatory equivalents for CO2(VE/VCO
References
sure decreased during the ascent. In contrast,
1. Burtscher M, Faulhaber M, Flatz M, Likar R, Nachbauer W.
the periods of decreasing SaO2 with relatively
Effects of short-term acclimatization to altitude (3200 m) on
constant PetCO2 may indicate steady state
aerobic and anaerobic exercise performance. Int J Sports
VE/VCO2 despite decreasing inspiratory oxygen
Med 2006;27:629—35.
2. Ursino M, Magosso E, Avanzolini G. An integrated model of
(2) The pre-treatment with intermittent hypoxia
the human ventilatory control system: the response to hyper- capnia. Clin Physiol 2001;21:447—64.
and/or azetazolamide clearly modified the
3. Katayama K, Sato Y, Morotome Y, Shima N, Ispida K, Mori S,
SaO2 pattern observed under control condi-
et al. Intermittent hypoxia increases ventilation and SaO2
tions. Intermittent hypoxia is known to enhance
during hypoxic exercise and hypoxic chemosenitivity. J ApplPhysiol 2001;90:1431—40.
ated with an augmented sensory response of
4. Ainslie PN, Barach A, Cummings KJ, Murrell C, Ham-
lin M, Hellemans J. Cardiorespiratory and cerebrovascular
responses to acute poikilocapnic hypoxia following intermit-
Therefore, this likely explains the prolonged
tent and continuous exposure to hypoxia in humans. J Appl
constant SaO2 periods after pre-treatment with
Physiol 2007;102:1953—61.
intermittent hypoxia. On the other hand, the
5. Swenson ER. Carbonic anhydrase inhibitors and ventilation: a
metabolic acidosis produced by acetazolamide
complex interplay of stimulation and suppression. Eur Respir J 1998;12:1242—7.
administration stimulates breathing at least
6. Jonk AM, van den Berg IP, Olfert IM, Wray DW, Arai T, Hop-
partly by increasing the tonic output of the cen-
kins SR, et al. Effect of acetazolamide on pulmonary and
muscle gas exchange during normoxic and hypoxic exercise.
the flattening of the decreasing SaO2 periods. J Physiol 2007;579:909—21.
7. Peng Y, Kline DD, Dick TE, Prabhakar NR. Chronic intermittent
But it cannot entirely be excluded that small
hypoxia enhances carotid body chemoreceptor response to
changes in the ascent rate may have influenced
low oxygen. Adv Exp Med Biol 2001;499:33—8.
Available online at www.sciencedirect.com
Please cite this article in press as: Burtscher M, Arterial oxygen saturation during ascending to altitude under variousconditions: Lessons from the field, J Sci Med Sport (2007), doi:
MATERIAL SAFETY DATA SHEET SECTION I - IDENTIFICATION L&M CONSTRUCTION CHEMICALS, INC NAME: LiON HARD SECTION II - HAZARDOUS INGREDIENTS/IDENTITY INFORMATION INGREDIENTS Listed and unlisted ingredients are not “hazardous” per OSHA Standard 29 CFR 1910.1200. SECTION III - PHYSICAL/CHEMICAL CHARACTERISTICS BOILING POINT (F): 214-216 (water-based) SECTI
Great Health. Generation to Generation. You are scheduled to have a surgical procedure at Garden City Hospital. • You must call the Pre-Registration department at 734-458-4408 with your insurance information at least one week prior to your scheduled surgery between 8 a.m. and 4 p.m., Monday through Friday. • After you have pre-registered, you will receive a call from a nurse in the Pre-Ad
 ARTICLE IN PRESS
ARTICLE IN PRESS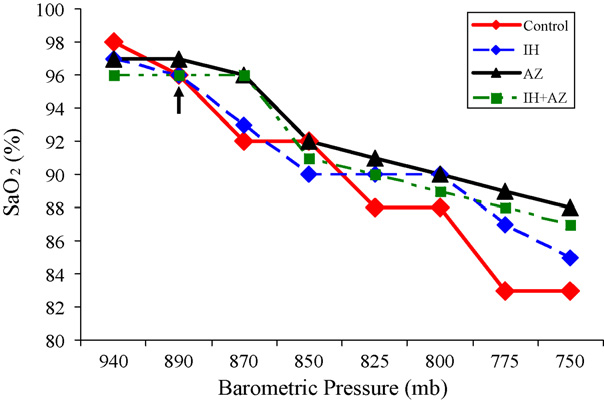 ARTICLE IN PRESS
ARTICLE IN PRESS